Conventioinal MRI Finding in a Case of Adhesive Shoulder Capsulitis
- Affiliations
-
- 1Department of Radiology, Yeosu Hanyeoexpo Hospital, Korea. parkharkhoon@hanmail.net
- 2Department of Orthopedic Surgery, Yeosu Baek Hospital, Korea.
- KMID: 2208887
- DOI: http://doi.org/10.3348/jksr.2010.63.1.57
Abstract
- PURPOSE
To evaluate the conventional magnetic resonance image findings in patients with adhesive shoulder capsulitis.
MATERIALS AND METHODS
The preoperative MR images of 76 patients with adhesive shoulder capsulitis that was also treated by arthroscopic capsule release. In contrast to the MR images of 25 control patients without adhesive shoulder capsulitis, the thickness and area of hyposignal intensity around the coracohumeral ligament (CHL), subcoracoidal fat, capsular thickness of the rotator interval, capsular thickness, and height of the axillary recess were measured. The existence of fluid in the axillary recess was also verified.
RESULTS
Patients with adhesive capsulitis showed a significant increase in the thickness (average 10.57 mm vs. 5.88 mm, T=8.289, p< 0.001), area (average 3.49 point vs. 0.96 point Z=7.775, p< 0.001) of hyposignal intensity around CHL, and a thickened joint capsule in the rotator interval (average 5.93 mm vs. 2.15 mm, Z=6.472, p< 0.001). The thickness of the hyposignal intensity around the CHL is about 10 mm or more and has a specificity of 96%, a sensitivity of about 55% in the area of hyposignal intensity from around the CHL, Seventy-five percent or more of cases, showed a 100%, 95%, complete obliteration of the subcoracoidal fat that was 96%, and a 50% thickness of the capsule. A rotator interval of 6mm or more had a 96%, 50% for the diagnosis of adhesive capsulitis of the shoulder. The capsular thickness and maximal height of axillary recess and the presence of fluid in the axillary recess was not significant in patients with adhesive shoulder capsulitis.
CONCLUSION
Thickening of the hyposignal intensity around the CHL, subcoracoidal fat obliteration, and capsular thickening at the rotator interval, are characteristic MRI findings in adhesive shoulder capsulitis.
MeSH Terms
Figure
-

Fig. 1 Scheme of measurement A. Thickest portion of hyposignal intensity around coracohumeral ligament on oblique sagittal T2-weighted images was measured (arrows). B. Thickest portion of thickened capsule around biceps long head tendon in rotator interval (= capsular thickness in rotator interval) was measured (arrows) on oblique sagittal T2-weighted images. C. Thickest portion of capsule (horizontal arrows) and maximal height of axillary recess (vertical arrows) were measured on oblique coronal T2-weighted image. Existence of joint fluid was checked also.

Fig. 2 Line drawings (top row) and corresponding oblique sagittal T2-weighted images (bottom row) of distribution of hyposignal intensity around coracohumeral ligament (CHL). A. Normal anatomy (arrows) in a subject without adhesive capsulitis (score 0). B. Distribution of hyposignal intensity around CHL was 25-50% to entire CHL (arrows) in a subject without adhesive capsulitis (score 2). Thickness of hyposignal intensity around CHL was 6.6 mm and capsular thickness in rotator interval was 2 mm. C. Distribution of hyposignal intensity around CHL was 51-75% to entire CHL(arrows) in a patient with adhesive capsulitis (score 3). Thickness of hyposignal intensity around CHL was 9.7 mm and capsular thickness in rotator interval was 6.3 mm. D. Distribution of hyposignal intensity around CHL was 76-100% to entire CHL (arrows) in a patient with adhesive capsulitis (score 4). Thickness of hyposignal intensity around CHL was 13 mm and capsular thickness in rotator interval was 9.3 mm.
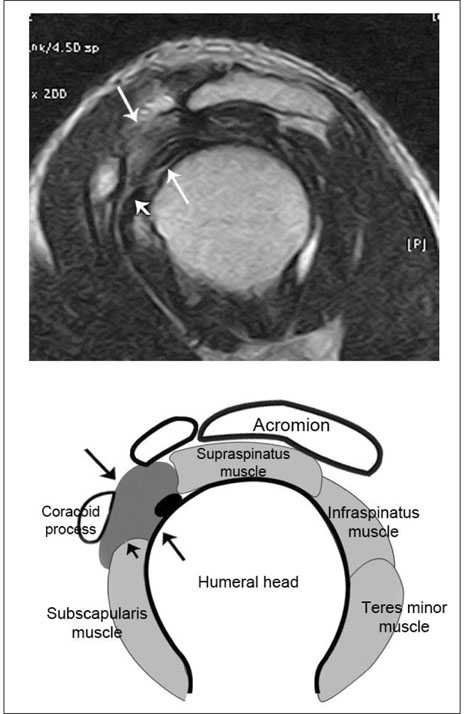
Fig. 3 Adhesive capsulitis on oblique sagittal T2-weighted image Capsular thickness in rotator interval was measured 9.3 mm (long arrows) in a patient with adhesive capsulitis. Distribution of hyposignal intensity around coracohumeral ligament (CHL) was 4 point, thickness of hyposignal intensity around CHL was checked 16 mm and subcoracoidal fat was obliterated completely (short arrows).
Reference
-
1. Carrillon Y, Noel E, Fantino O, Perrin-Fayolle O, Tran-Minh VA. Magnetic resonance imaging findings in idiopathic adhesive capsulitis of the shoulder. Rev Rhum Engl Ed. 1999; 66:201–206.2. Warner JJ. Frozen Shoulder: Diagnosis and Management. J Am Acad Orthop Surg. 1997; 5:130–140.3. Park TS, Na JU, Kim SI, Kim TS. Arthroscopic management and manipulation of chronic idiopathic adhesive capsulitis of the shoulder. J Korean Orthop Assoc. 2001; 36:367–371.4. Codman EA. Tendinitis of the short rotators. In : Codman EA, editor. The Shoulder, Ruptures of the supraspinatus tendon and other lesions on or about the subacromial bursa. Boston, Mass: Thomas Todd;1934.5. Neviaser JS. Adhesive capsulitis of the shoulder: a study of the pathologic findings in periarthritis of the shoulder. J Bone Joint Surg Am. 1945; 27:211–222.6. Uitvlugt G, Detrisac DA, Johnson LL, Austin MD, Johnson C. Arthroscopic observations before and after manipulation of frozen shoulder. Arthroscopy. 1993; 9:181–185.7. Jeon JM. Evaluation, Differential Diagnosis of the Painful Shoulder. Clin Shoulder Elb. 2003; 6:15–21.8. Shaffer B, Tibone JE, Kerlan RK. Frozen shoulder: a long-term follow-up. J Bone Joint Surg Am. 1992; 74:738–746.9. Matsen III FA, Lippitt SB, Sidles JA, Harryman II DT. Practical evaluation of management of the shoulder. Philadelphia: W.B. Saunders;1994. p. 19–109.10. Neer CS 2nd, Satterlee CC, Dalsey RM, Flatow EL. The anatomy and potential effects of contracture of the coracohumeral ligament. Clin Orthop Relat Res. 1992; (280):182–185.11. Warner JJ, Allen A, Marks PH, Wong P. Arthroscopic release for chronic, refractory adhesive capsulitis of the shoulder. J Bone Joint Surg Am. 1996; 78:1808–1816.12. Ozaki J, Nakagawa Y, Sakurai G, Tamai S. Recalcitrant chronic adhesive capsulitis of the shoulder: role of contracture of the coracohumeral ligament and rotator interval in pathogenesis and treatment. J Bone Joint Surg Am. 1989; 71:1511–1515.13. Omari A, Bunker TD. Open surgical release for frozen shoulder: surgical findings and results of the release. J Shoulder Elbow Surg. 2001; 10:353–357.14. Kim HJ, Han TI, Lee KW, Kwon ST, Choi YS, Kim DH, Han HY, Song MK. Adhesive Capsulitis of the Shoulder: MR Arthrography. J Korean Radiol Soc. 2001; 45:55–59.15. Wiley AM. Arthroscopic appearance of frozen shoulder. Arthroscopy. 1991; 7:138–143.16. Mengiardi B, Pfirrmann CW, Gerber C, Hodler J, Zanetti M. Frozen Shoulder: MR arthrographic findings. Radiology. 2004; 233:486–492.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Adhesive Capsulitis of the Shoulder
- The Effects of Stellate Ganglion Block in Adhesive Capsulitis of the Shoulder
- The Comparison of Therapeutic Effect of Shoulder Pain with Simple and Mixed Type in Patients with Adhesive Capsulitis
- Ultrasonography in Adhesive Capsulitis of Shoulder
- Limited Joint Motion in Type II Diabetic Patients; Association with Diabetic Complications and Related Disease
