Usefulness of Angiographic Embolization after Endoscopic Metallic Clip Placement in Patient with Non-Variceal Upper Gastrointestinal Bleeding
- Affiliations
-
- 1Department of Radiology, Konyang University Hospital, Daejeon, Korea. hushymj@hanmail.net
- 2Department of Radiology, Chungnam National University College of Medicine, Daejeon, Korea.
- 3Department of Radiological Science, Konyang University, Daejeon, Korea.
- 4Department of Radiology, Inje University College of Medicine, Pusan Paik Hospital, Busan, Korea.
- KMID: 2208815
- DOI: http://doi.org/10.3348/jksr.2013.69.2.123
Abstract
- PURPOSE
The aim of this study is to assess the usefulness of angiographic embolization after endoscopic metallic clip placement around the edge of non-variceal upper gastrointestinal bleeding ulcers.
MATERIALS AND METHODS
We have chosen 41 patients (mean age, 65.2 years) with acute bleeding ulcers (22 gastric ulcers, 16 duodenal ulcers, 3 malignant ulcers) between January 2010 and December 2012. We inserted metallic clips during the routine endoscopic treatments of the bleeding ulcers. Subsequent transcatheter arterial embolization was performed within 2 hours. We analyzed the angiographic positive rates, angiographic success rates and clinical success rates.
RESULTS
Among the 41 patients during the angiography, 19 patients (46%) demonstrated active bleeding points. Both groups underwent embolization using microcoils, N-butyl-cyano-acrylate (NBCA), microcoils with NBCA or gelfoam particle. There are no statistically significant differences between these two groups according to which embolic materials are being used. The bleeding was initially stopped in all patients, except the two who experienced technical failures. Seven patients experienced repeated episodes of bleeding within two weeks. Among them, 4 patients were successful re-embolized. Another 3 patients underwent gastrectomy. Overall, clinical success was achieved in 36 of 41 (87.8%) patients.
CONCLUSION
The endoscopic metallic clip placement was helpful to locate the correct target vessels for the angiographic embolization. In conclusion, this technique reduced re-bleeding rates, especially in patients who do not show active bleeding points.
MeSH Terms
Figure
-

Fig. 1 A 64-year-old man who presented with massive upper gastrointestinal bleeding. A. About 5 cm in size, large ulcer covered with hematoma and whitish plaque at greater curvature side of gastric body on endoscopy. B. There is no definite bleeding site on left gastric artery angiography. C. Super-selective angiography using microcatheter demonstrates extravasation (arrow) from one of the branches of left gastric artery. D. After embolization using microcoils (arrow). No visible extravasation is noted on post-embolization angiography. E. 3 weeks later, the follow-up endoscopy shows no hemorrhagic plaque nor active hemorrhage and the atrophic change of the ulcer is noted.

Fig. 2 A 79-year-old man who presented with gastric ulcer. A. On endoscopy, there is active ulcer in lesser curvature side of mid-body of stomach, with dark hematoma around ulcer mound. B. No evidence of active extravasation on angiography, but we performed super-selective angiographic embolization using micro-coils around metallic clips. C. Two days after the follow-up endoscopy, there is trace of bleeding (arrow) at ulcer site but no active bleeding is noted. D. One day after the endoscopy, he presented with large amount of melena and unstable vital sign. Subsequent 2nd angiography demonstrates recanalization (open arrows) of distal portion of the previous embolization coil (white arrow) and we performed re-embolization which was successful.
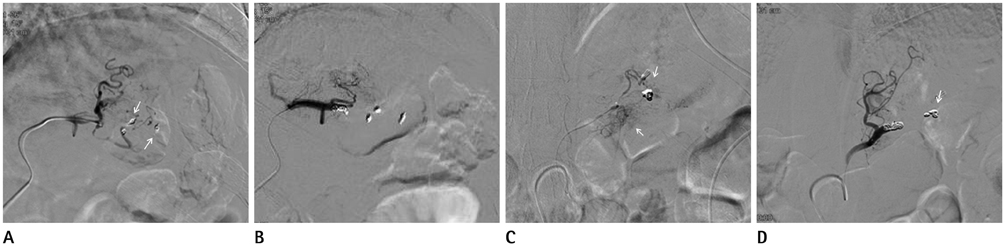
Fig. 3 A 51-year-old man who presented with gastric ulcer bleeding on endoscopy. A. There is active bleeding site from branch vessels of left gastric artery toward metallic clips (arrows) on microangiography. B. Angiographic embolization of these vessels using microcoil. C. 5 days after embolization, re-bleeding is noted on the follow-up endoscopy. We performed angiography, demonstrating bleeding (arrows) from surrounding collateral vessels toward metallic clips. D. Successful embolization using the additional micro-coil (arrow).
Reference
-
1. Rockall TA, Logan RF, Devlin HB, Northfield TC. Incidence of and mortality from acute upper gastrointestinal haemorrhage in the United Kingdom. Steering Committee and members of the National Audit of Acute Upper Gastrointestinal Haemorrhage. BMJ. 1995; 311:222–222.2. British Society of Gastroenterology Endoscopy Committee. Non-variceal upper gastrointestinal haemorrhage: guidelines. Gut. 2002; 51:Suppl 4. iv1–iv6.3. Saltzman JR, Strate LL, Di Sena V, Huang C, Merrifield B, Ookubo R, et al. Prospective trial of endoscopic clips versus combination therapy in upper GI bleeding (PROTECCT--UGI bleeding). Am J Gastroenterol. 2005; 100:1503–1508.4. Binmoeller KF, Thonke F, Soehendra N. Endoscopic hemoclip treatment for gastrointestinal bleeding. Endoscopy. 1993; 25:167–170.5. Longstreth GF. Epidemiology of hospitalization for acute upper gastrointestinal hemorrhage: a population-based study. Am J Gastroenterol. 1995; 90:206–210.6. Loffroy R, Rao P, Ota S, De Lin M, Kwak BK, Geschwind JF. Embolization of acute nonvariceal upper gastrointestinal hemorrhage resistant to endoscopic treatment: results and predictors of recurrent bleeding. Cardiovasc Intervent Radiol. 2010; 33:1088–1100.7. Hung CF, Cheng TL, Wu RH, Teng CF, Chang WT. A novel bidirectional expression system for simultaneous expression of both the protein-coding genes and short hairpin RNAs in mammalian cells. Biochem Biophys Res Commun. 2006; 339:1035–1042.8. Rupp T, Singh S, Waggenspack W. Gastrointestinal hemorrhage: the prehospital recognition, assessment & management of patients with a GI bleed. JEMS. 2004; 29:80–81. 83–95. quiz 96–quiz 97.9. Schenker MP, Duszak R Jr, Soulen MC, Smith KP, Baum RA, Cope C, et al. Upper gastrointestinal hemorrhage and transcatheter embolotherapy: clinical and technical factors impacting success and survival. J Vasc Interv Radiol. 2001; 12:1263–1271.10. Aina R, Oliva VL, Therasse E, Perreault P, Bui BT, Dufresne MP, et al. Arterial embolotherapy for upper gastrointestinal hemorrhage: outcome assessment. J Vasc Interv Radiol. 2001; 12:195–200.11. Jae HJ, Chung JW, Jung AY, Lee W, Park JH. Transcatheter arterial embolization of nonvariceal upper gastrointestinal bleeding with N-butyl cyanoacrylate. Korean J Radiol. 2007; 8:48–56.12. Lang EK. Transcatheter embolization in management of hemorrhage from duodenal ulcer: long-term results and complications. Radiology. 1992; 182:703–707.13. Song JS, Kwak HS, Chung GH. Nonvariceal upper gastrointestinal bleeding: the usefulness of rotational angiography after endoscopic marking with a metallic clip. Korean J Radiol. 2011; 12:473–480.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Nonvariceal Upper Gastrointestinal Bleeding: the Usefulness of Rotational Angiography after Endoscopic Marking with a Metallic Clip
- Endoscopic Management of Gastrointestinal Leaks and Bleeding with the Over-the-Scope Clip: A Prospective Study
- Endoscopic Hemostasis for Non-Variceal Upper Gastrointestinal Bleeding: New Frontiers
- Recent Update of Embolization of Upper Gastrointestinal Tract Bleeding
- Endoscopic Treatment and Prevention of Acute Variceal Hemorrhage
