Polyarteritis Nodosa in Superior Mesenteric Artery: A Case Report
- Affiliations
-
- 1Department of Radiology, Pathology, Hallym University College of Medicine.
- KMID: 2201399
- DOI: http://doi.org/10.3348/jkrs.1998.38.3.441
Abstract
- Polyarteritis nodosa(PAN) is a multisystem disease characterized by necrotizing vasculitis of small andmedium-sized arteries, and in 50% of all cases there is gastrointestinal involvement. We describe a patient withPAN involving the gastrointestinal tract. A small bowel series showed nodular fold thickening, submucosal fillingdefects, shallow ulcerations, segmental luminal narrowing, and decreased peristalsis at the duodenum, jejunum, andileum; superior mesenteric arteriography showed hypervascularity and microaneurysm. Segmental resection of thesmall bowel indicated the presence of PAN.
Keyword
MeSH Terms
Figure
-
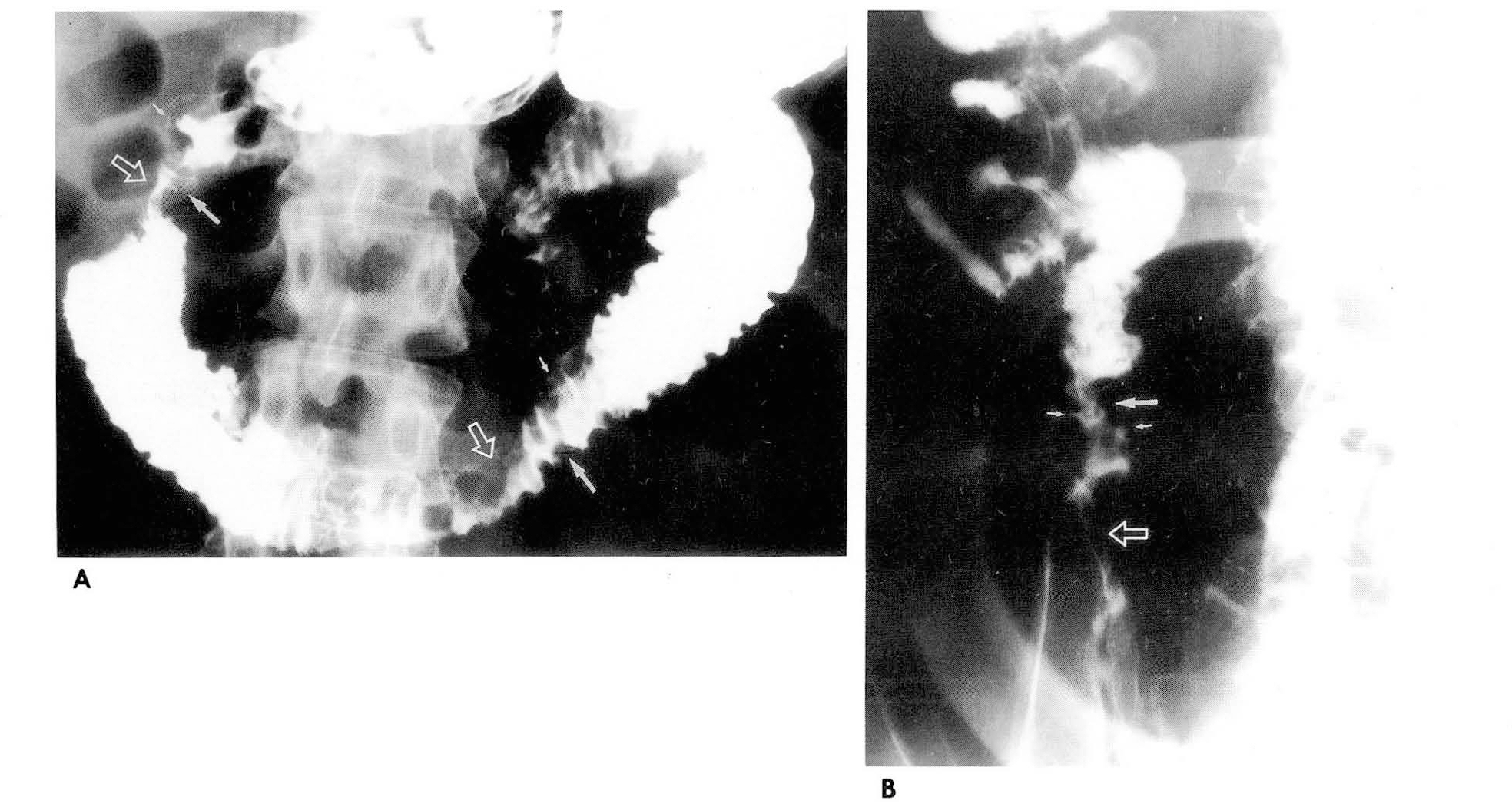
Fig. 1. Small bowel series shows submucosal filling defects (large arrows), shallow ulcerations (small arrows), and multiple segmental luminal narrowing (open arrows) in duodenum(A) and terminal il- eum(B).

Fig. 2. Hypervascularity and numerous microaneurysms (arrows) are noted at jejunal(A) and ilea 1(B) branch of superior mesenteric artery on arterial phase of arteriogram. Small contrast poolings (arrows) are noted at ileal branches on venous phase of superior mesenteric arteriography(C).

Fig. 3. A. Photomicrograph shows ulceration and regeneration of the mucosa. There is aneurysmal dilatation of artery showing necrotizing inflammation in submucosa. (Η & Ε stain, X40) B. The artery in the serosa is occluded by thrombus and shows disruption and fragmentation of internal elastic lamina. (Elastic stain, X100)
Reference
-
1.Kussmaul A., Maier Κ. Uber eine bischer nicht beschreibene eigenthumliche Arterienerkrankung (Polyarteritis nodosa), die mit Morbus Brightii und rapid fortschreitender allgemeiner Muskellahmung einhergeht. Dtsch Arch Klin Med. 1:484–517. 1866.2.Cupps T., Fauci A. The vasculitidis. In: Cupps TR, Fauci AS, eds. Major problems in internal medicine. Vol 21. Philadelphia: WB Saunders. 1981.3.Lopez L., Schocket A., Stanford R, et al. Gastrointestinal involvement in leukocytoclastic vasculitis and polyarteritis nodosa. J Rheumatol. 1980. 5:677–687.4.McCouley R., Johnston M., Fauci A. Surgical aspects of systemic necrotizing vasculitis. Surgery. 1985. 97:104–110.5.Spiegel R. Clinical aspects of periarteritis nodosa. Arch Intern Med. 1936. 58:993–1040.
Article6.C. Craig T, Barry M.B. Renal pathology with clinical correlation and functional correlations,. 2nd ed.Philadelphia: Lippincott;1993. p. 1990–1993.7.Halpern M., Citron BP. Necrotizing angiitis associated with drug abuse. AJR. 1971. 3:663–671.
Article8.Hekali P.., Kajander H.., Pajari R., et al. Diagnostic significance of angiographically observed visceral aneurysms with regard to polyarteritis nodosa. Acta Radiol. 1991. 32:143–148.
Article9.Marshak RH., Lindner AE. Radiology of the small intestine, ed 2. Philadelphia. 1976. WB Saunders.10.Craig RDP. Multiple perforations of the small intestine in polyarteritis nodosa. Gastroenterology. 1963. 44:355.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hybrid Surgery to Treat Multiple Visceral Aneurysms Secondary to Polyarteritis Nodosa
- Failure of Conservative Treatment in Two Cases of Polyarteritis Nodosa with Superior Mesenteric Artery Involvement Presenting with Abdominal Pain
- A case of polyarteritis nodosa with bilateral ureteral obstruction
- A Case of Polyarteritis Nodosa Associated with Central Retinal Artery Occlusion
- Polyangiitis overlap syndrome: cutaneous leukocytoclastic vasculitis associated with polyarteritis nodosa
