Endovascular Embolization of a Ruptured Distal Lenticulostriate Artery Aneurysm in Patients with Moyamoya Disease
- Affiliations
-
- 1Department of Neurosurgery, Seoul National University Bundang Hospital, Seongnam, Korea. storynlemon@gmail.com
- KMID: 2191141
- DOI: http://doi.org/10.3340/jkns.2014.56.6.492
Abstract
- A ruptured distal lenticulostriate artery (LSA) aneurysm is detected occasionally in moyamoya disease (MMD) patients presented with intracerebral hemorrhage. If the aneurysm is detected in hemorrhage site on angiographic evaluation, its obliteration could be considered, because it rebleeds frequently, and is associated with poorer outcome and mortality in MMD related hemorrhage. In this case report, the authors present two MMD cases with ruptured distal LSA aneurysm treated by endovascular embolization.
MeSH Terms
Figure
-
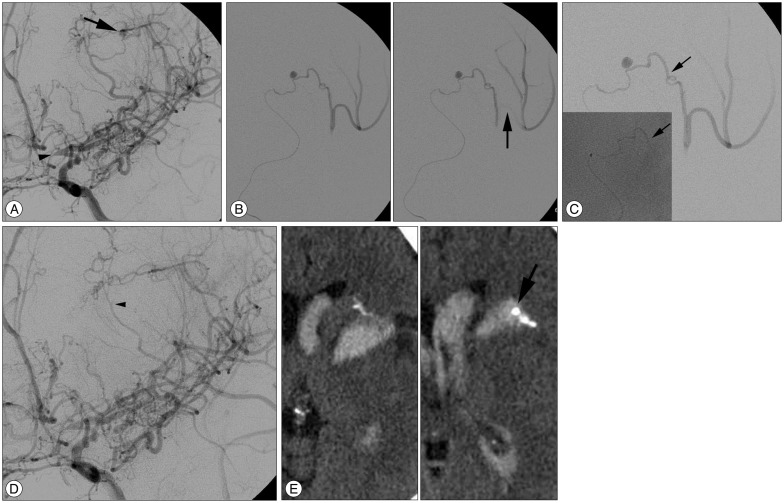
Fig. 1 A : A ruptured aneurysm (arrow) is located on a branch of the lenticulostriate artery (LSA), which connects this LSA with the insular branch of the M2 segments of left middle cerebral artery (MCA). The LSA is originated from the A1 segment of the anterior cerebral artery (arrowhead), which indicates that the LSA is a medial one. Distal medullary vessels from this LSA are also noted. B : The target branch with the ruptured aneurysm is selected directly with a microcatheter to save the distal medullary vessels. Selective angiogram shows the target branch and the MCA branches connected with it. These MCA branches disappear on selective angiogram after brief contrast opacification (arrow), suggesting other collateral flows. C : N-butyl-cyanoacrylate (NBCA) is injected into the target branch, not over the M2 segment. Arrows indicate the intended target point and the final glue endpoint. D : Postembolization angiogram shows patent flows of the medial LSA, its distal medullary vessels, and the MCA branches. The target branch with the aneurysm is no more seen except its stump (arrowhead). E : The target branch and aneurysm (arrow) filled with NBCA are observed on follow-up CT scan.
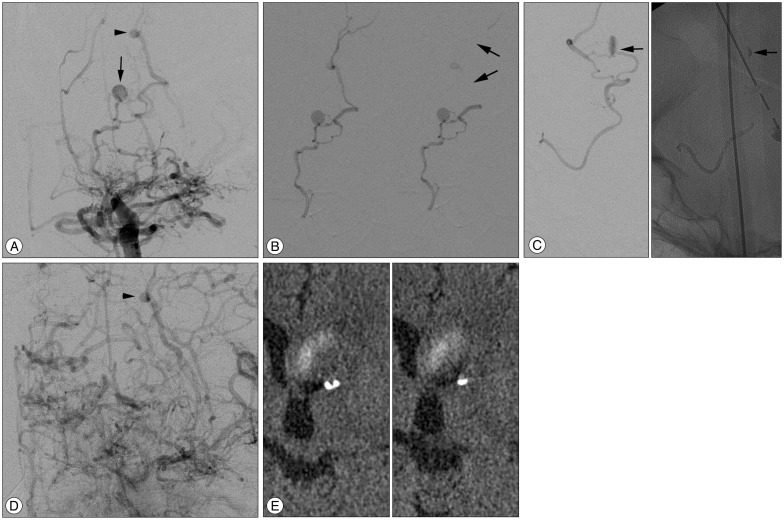
Fig. 2 A : A ruptured aneurysm (arrow) is noted in the distal lenticulostriate artery (LSA). Another aneurysmal dilatation (arrowhead) is also observed on a cortical vessel via distal medullary vessel from this LSA. B : Selective angiogram shows the aneurysm and the cortical branches. Contrast in the cortical branches washes out after brief opacification, suggesting that the LSA with the aneurysm is wedged with a microcatheter and its distal branches are supplied by blood flow via another collaterals (arrows). C : Treatment working view. N-butyl-cyanoacrylate (NBCA) is injected into the LSA up to the aneurysm (arrows). D : Postembolization angiogram shows complete obliteration of the aneurysm and patent flow of the distal cortical branches with the aneurysmal dilatation (arrowhead). E : NBCA filling in the LSA and aneurysm is detected on follow-up CT scan.
Cited by 1 articles
-
Recurrent Bleeding in Hemorrhagic Moyamoya Disease : Prognostic Implications of the Perfusion Status
Kyung-Il Jo, Min Soo Kim, Je Young Yeon, Jong-Soo Kim, Seung-Chyul Hong
J Korean Neurosurg Soc. 2016;59(2):117-121. doi: 10.3340/jkns.2016.59.2.117.
Reference
-
1. Chalouhi N, Tjoumakaris S, Gonzalez LF, Dumont AS, Shah Q, Gordon D, et al. Onyx embolization of a ruptured lenticulostriate artery aneurysm in a patient with moyamoya disease. World Neurosurg. 2013; 80:436.e7. 436.e10. PMID: 22484074.
Article2. Cho HJ, Roh HG, Moon WJ, Kim HY. Perforator territory infarction in the lenticulostriate arterial territory : mechanisms and lesion patterns based on the axial location. Eur Neurol. 2010; 63:107–115. PMID: 20090345.
Article3. Harreld JH, Zomorodi AR. Embolization of an unruptured distal lenticulostriate aneurysm associated with moyamoya disease. AJNR Am J Neuroradiol. 2011; 32:E42–E43. PMID: 20075103.
Article4. Kim SH, Kwon OK, Jung CK, Kang HS, Oh CW, Han MH, et al. Endovascular treatment of ruptured aneurysms or pseudoaneurysms on the collateral vessels in patients with moyamoya disease. Neurosurgery. 2009; 65:1000–1004. discussion 1004. PMID: 19834414.
Article5. Larrazabal R, Pelz D, Findlay JM. Endovascular treatment of a lenticulostriate artery aneurysm with N-butyl cyanoacrylate. Can J Neurol Sci. 2001; 28:256–259. PMID: 11513346.
Article6. Nah HW, Kwon SU, Kang DW, Ahn JS, Kwun BD, Kim JS. Moyamoya disease-related versus primary intracerebral hemorrhage : [corrected] location and outcomes are different. Stroke. 2012; 43:1947–1950. PMID: 22693130.
Article7. Saeki N, Nakazaki S, Kubota M, Yamaura A, Hoshi S, Sunada S, et al. Hemorrhagic type moyamoya disease. Clin Neurol Neurosurg. 1997; 99(Suppl 2):S196–S201. PMID: 9409437.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Ruptured lenticulostriate artery aneurysm in moyamoya disease treated with Onyx embolization
- Successful Endovascular Treatment of Ruptured Superior Cerebellar Artery Aneurysm Associated with Moyamoya Disease : A Case Report and Review of the Literature
- Ruptured Distal Lenticulostriate Artery Aneurysm Associated with Ipsilateral Middle Cerebral Artery Occlusion : Case Report
- Coil Embolization for Distal Middle Cerebral Artery Aneurysm
- Coil Embolization of Ruptured Thrombosed Distal Superior Cerebellar Artery Aneurysm: A Case Report
