New Fibular Strut Graft Technique to Minimize Donor Site Complications
- Affiliations
-
- 1Department of Orthopedics, Chonnam National University Hospital, Gwangju, Korea. stjung@chonnam.ac.kr
- KMID: 2186550
- DOI: http://doi.org/10.4055/jkoa.2007.42.3.285
Abstract
-
PURPOSE: To evaluate the effectiveness of a periosteal sleeve preserced fibular strut graft for the minimization of donor site complications.
MATERIALS AND METHODS
Between September 1998 and March 2005, 20 patients who were followed for more than 12 months after the fibular sturt graft for a bone defect using a periosteal sleeve preservation technique were evaluated. The mean age was 13.3 years (range, 2-29 years) and the mean follow-up period was 16.2 months (range, 12-36 months).
RESULTS
The mean time for the union of the primary disease was 3.3 months (range, 2-6 months) and for regeneration of the donor site was 9.1 weeks (range, 4-12 weeks) in 13 cases. Partial regeneration developed in 6 cases and there was no regeneration in 1 case. There were 2 cases of donor site complications.
CONCLUSION
The new fibular strut graft technique is very effective method for reconstruction of a bone defect with a minimization of the donor site complications particularly in children.
Figure
-
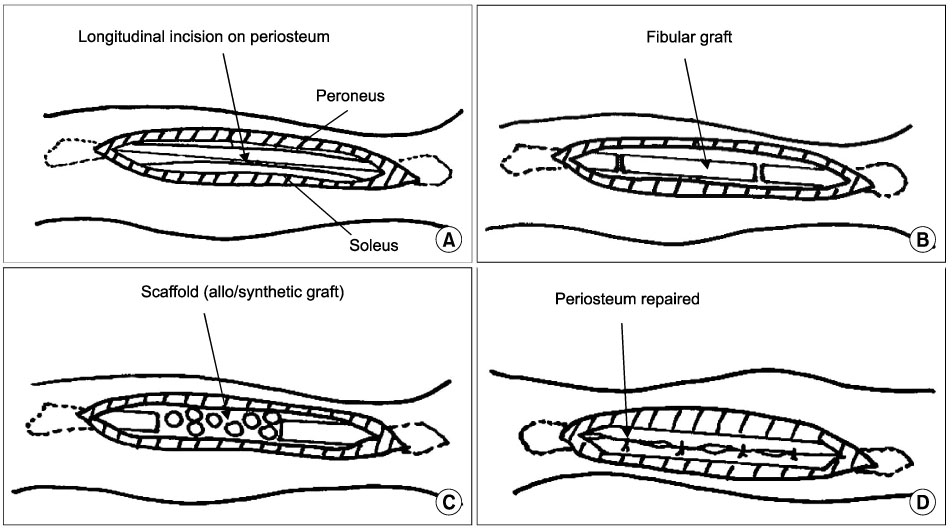
Fig. 1 (A) A longitudinal incision was made on the fibular and its periosteum. (B) The fibular was harvested using a periosteal preservation technique. (C) Bone defect of the donor site was filled with an allochip graft or calcium sulfate. (D) The periosteum was sutured.

Fig. 2 A) Preoperative radiograph of a 6-year-old boy show a simple bone cyst on the proximal femur. (B) Immediate postoperative radiograph show a bone defect of the primary disease filled with fibula. A new defect of donated fibular was filled with an allochip graft and repaired using a periosteal preservation technique. (C) After 3 months, the primary disease was healed and the fibular had completely regenerated.
Cited by 1 articles
-
Treatment of Metaphyseal Pathologic Fractures of Long Bone Using Locking Compression Plate in Children
Sung-Taek Jung, Kwang-Cheul Jeong, Hyun-Jong Kim, Jin-Ho Lee
J Korean Orthop Assoc. 2008;43(5):539-543. doi: 10.4055/jkoa.2008.43.5.539.
Reference
-
1. Chapman MW, Rodrigo JJ. Bone grafting, bone graft substitutes, and growth factors. Chapman's orthopedic surgery. 1993. 3rd ed. Lippincott Williams & Wilkins;181–215.2. Chen MT, Chang MC, Chen CM, Chen TH. Double-strut free vascular fibular grafting for reconstruction of the lower extremities. Injury. 2003. 34:763–769.
Article3. Ganel A, Yaffe B. Ankle instability of the donor site following removal of vascularized fibular bone graft. Ann Plast Surg. 1990. 24:7–9.4. Gitelis S, Piasecki P, Turner T, Haggard W, Charters J, Urban R. Use of a calcium sulfate-based bone graft substitute for benign bone lesions. Orthopedics. 2001. 24:162–166.
Article5. Hatori M, Ayoub KS, Grimer RJ, Carter SR, Tillman RM. The two-stage ipsilateral fibular transfer for tibial defect following tumour excision. Sarcoma. 2000. 4:27–30.
Article6. Kerry RM, Masri BA, Garbuz DS, Czitrom A, Duncan CP. The biology of bone grafting. Instr Course Lect. 1999. 48:645–652.7. Kim HM, Lee KH, Jeong CH, Kim YS, Choi MG, Ilm IJ. Treatment of avascular necrosis of the femoral head with free vascularized fibular graft. J Korean Orthop Assoc. 1998. 33:941–951.
Article8. Lee EH, Goh JC, Helm R, Pho RW. Donor site morbidity following resection of the fibula. J Bone Joint Surg Br. 1990. 72:129–131.
Article9. Meagher PJ, Morrison WA. Free fibula flap-donor-site morbidity: case report and review of the literature. J Reconstr Microsurg. 2002. 18:465–468.
Article10. Mirzayan R, Panossian V, Aveldian R, Forrester DM, Menendez LR. The use of calcium sulfate in the treatment of benign bone lesions. A preliminary report. J Bone Joint Surg Am. 2001. 83:355–358.11. Peltier LF, Jones RH. Treatment of unicameral bone cysts by curettage and packing with plaster-of-Paris pellets. J Bone Joint Surg Am. 1978. 60:820–822.
Article12. Rougraff BT. Bone graft alternatives in the treatment of benign bone tumors. Instr Course Lect. 2005. 54:505–512.13. Shpitzer T, Neligan P, Boyd B, Gullane P, Gur E, Freeman J. Leg morbidity and function following fibular free flap harvest. Ann Plast Surg. 1997. 38:460–464.
Article14. Vogelin E, Jones NF, Huang JI, Brekke JH, Lieberman JR. Healing of a critical-sized defect in the rat femur with use of a vascularized periosteal flap, a biodegradable matrix, and bone morphogenetic protein. J Bone Joint Surg Am. 2005. 87:1323–1331.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ankle Arthrodesis by Internal Fixation with Cancellous Screws and Fibula Strut Graft: Report of Two Cases
- Total Hip Arthroplasty in the Severely Narrowed Femoral Canal by a Fibular Strut Using Knee Arthroscopic Tools: A Case Report and Technical Note
- Intramedullary fibula strut bone allograft in a periprosthetic humeral shaft fracture with implant loosening after total elbow arthroplasty
- Anterior Fibular Strut Graft in the Treatment of Cervical Spinal Cord Injury: Case Report
- A Comparative Study of Donor Site Morbidity between Patients with or without Iliac Donor Site Reconstruction after Anterior Thoracolumbar Spinal Fusion using Auto-Iliac Tricortical Strut done Graft.
