J Korean Orthop Assoc.
2014 Feb;49(1):74-78. 10.4055/jkoa.2014.49.1.74.
Musculocutaneous Nerve Entrapment after Biceps Long Head Tendon Rupture
- Affiliations
-
- 1Department of Orthopedic Surgery, Inha University School of Medicine, Incheon, Korea. tjlee@inha.ac.kr
- KMID: 2185261
- DOI: http://doi.org/10.4055/jkoa.2014.49.1.74
Abstract
- Biceps long head tendon rupture is relatively common and requires approximately four weeks of splintage as a general treatment. Musculocutaneous nerve entrapment is commonly caused by excessive exercise or direct external force. Musculocutaneous nerve syndrome has barely been reported; however, association of biceps long head tendon rupture and musculocutaneous nerve entrapment syndrome has never been reported. The authors experienced a 70-year-old male patient, who suffered a traffic accident and was hospitalized due to shoulder joint pain caused by direct external force, delayed forearm lateral aspect hypoesthesia and elbow flexion weakness. For identification of the cause, magnetic resonance imaging, electromyography, and surgical opinion were synthesized, resulting in diagnosis of delayed musculocutaneous nerve entrapment syndrome occurring after biceps long head tendon rupture. With surgical treatment, pain, sense, and elbow flexion weakness were recovered, a showing successful treatment result.
MeSH Terms
Figure
-

Figure 1 T2-weighted magnetic resonance imaging coronal section, biceps brachii long head tendon (thin arrow) ruptured and distracted from humerus great tuberosity approximately 12 cm.
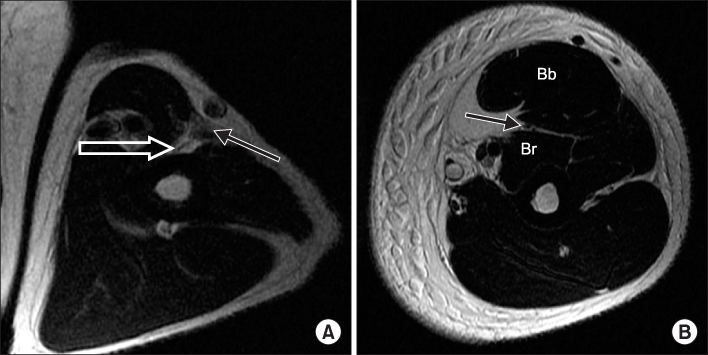
Figure 2 T2-weighted magnetic resonance imaging axial section, (A) migrated biceps brachii (Bb) long head tendon (thick arrow) located just next to the musculocutaneous nerve (thin arrow) at the left mid-arm level in this patient. (B) Normal musculocutaneous nerve (thin arrow) observed between Bb muscle and brachialis muscle (Br) at the left mid-arm level.
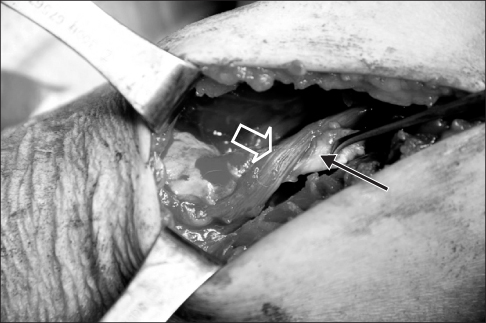
Figure 3 Intraoperative finding. Ruptured biceps brachii long head tendon (thin arrow) adhered with musculocutaneous nerve (thick arrow) at lt. Mid-arm level.
Reference
-
1. Yilmaz C, Eskandari MM, Colak M. Traumatic musculocutaneous neuropathy: a case report. Arch Orthop Trauma Surg. 2005; 125:414–416.
Article2. Dailiana ZH, Roulot E, Le Viet D. Surgical treatment of compression of the lateral antebrachial cutaneous nerve. J Bone Joint Surg Br. 2000; 82:420–423.
Article3. Felsenthal G, Mondell DL, Reischer MA, Mack RH. Forearm pain secondary to compression syndrome of the lateral cutaneous nerve of the forearm. Arch Phys Med Rehabil. 1984; 65:139–141.4. Ma H, Van Heest A, Glisson C, Patel S. Musculocutaneous nerve entrapment: an unusual complication after biceps tenodesis. Am J Sports Med. 2009; 37:2467–2469.5. Krupp RJ, Kevern MA, Gaines MD, Kotara S, Singleton SB. Long head of the biceps tendon pain: differential diagnosis and treatment. J Orthop Sports Phys Ther. 2009; 39:55–70.
Article6. Neal S, Fields KB. Peripheral nerve entrapment and injury in the upper extremity. Am Fam Physician. 2010; 81:147–155.7. Tagliafico AS, Michaud J, Marchetti A, Garello I, Padua L, Martinoli C. US imaging of the musculocutaneous nerve. Skeletal Radiol. 2011; 40:609–616.
Article8. Pećina M, Bojanić I. Musculocutaneous nerve entrapment in the upper arm. Int Orthop. 1993; 17:232–234.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Reconstruction of chronic long head of biceps tendon tears with gracilis allograft: report of two cases
- Intratendinous Ganglion of the Long Head of the Biceps Tendon
- Bilateral Congenital Absence of the Long Head of Biceps Brachii Tendon in Shoulder Joints: A case report
- Increased Biceps Translation: A Clinical Sign of Complete Distal Biceps Tendon Rupture
- Accessory Tendon of Biceps Brachii Originated from Pectoralis Major
