Basic Principles and Current Trends of Medial Opening-Wedge High Tibial Osteotomy
- Affiliations
-
- 1Department of Orthopaedic Surgery, Korea University Anam Hospital, Korea University College of Medicine, Seoul, Korea. oshan@korea.ac.kr
- KMID: 2185213
- DOI: http://doi.org/10.4055/jkoa.2014.49.2.85
Abstract
- High tibial osteotomy (HTO) is a popular surgical procedure for osteoarthritis of the knee with varus deformity. In general, HTO has shown sufficient clinical outcomes with careful patient selection and correct surgical technique. Among various surgical techniques, medial opening-wedge and lateral closing-wedge HTO are widely used. This report includes basic principles and current trends in patient selection and preoperative evaluations and planning, operative technique, complications, and rehabilitation protocol in medial opening-wedge HTO.
Figure
-
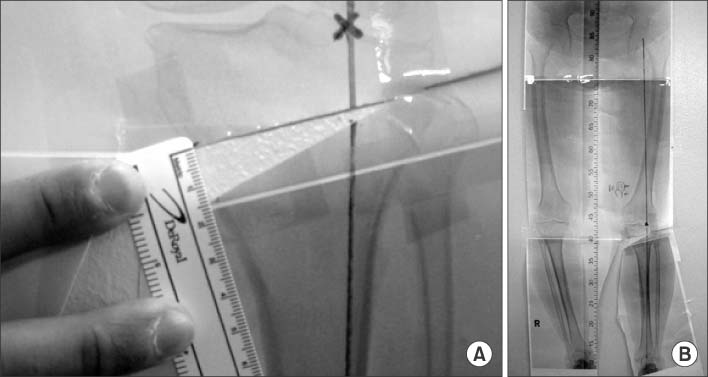
Figure 1 Scanography measurement method. A template was cut through the osteotomy site and the tibia was rotated until the weight-bearing line passed through the 62% coordinate.

Figure 2 Bilateral weight bearing anteroposterior whole lower limb X-ray in full extension for planning an open wedge high tibial osteotomy. (A) Method by Miniaci (Line 1 represents the planned weight bearing line for the postoperative correction extending from the center of the hip through a coordinate 60%-70% of the tibial plateau width past the ankle. Line 2 connects the osteotomy hinge point with the center of the ankle. Line 3 connects the osteotomy hinge point with the arc intersection of line 1. The angle formed by lines 2 and 3 is the planned correction angle (x)). (B) Method by Dugdale and Noyes (Line 1 is drawn from the center of the femoral head to the 62.5% of the tibial width. Line 2 is drawn from the center of the tibiotalar joint to the 62.5% coordinate. The angle formed by these two lines is the correction angle (x)). (C) Method by Conventry.

Figure 3 Anteroposterior radiograph of the knee showing the extent of the safe zone. Between A and B: safe zone. A, tip of the fibular head; B, circumference line of the fibular head.

Figure 4 The dorsal cut of the biplanar osteotomy also started 4 cm below the medial joint line. Only the posterior two thirds of the tibia were cut. The frontal third of the tibia was left intact. The anterior cut was aimed at a point 2 cm below the ventral joint line.

Figure 5 Clinical picture shows that pes anserinus is pulled distally from its head edge using a hook after separating the subcutaneous tissue and fascia.
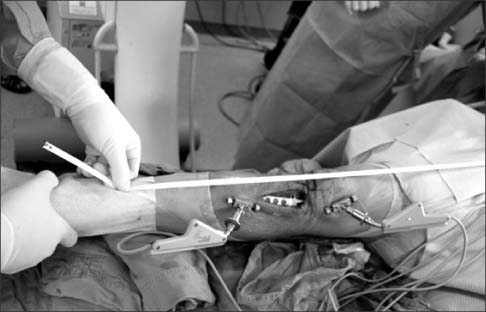
Figure 6 Clinical photo shows intraoperative finding that the mechanical axis can be evaluated using Bovie line or a measuring tape.

Figure 7 Preoperative (A) and postoperative (B) anteroposterior whole lower limb X-ray.
Cited by 1 articles
-
Osteotomy around the Knee: Indication and Preoperative Planning
Seung Wan Lim, Seung Min Ryu, Oog Jin Shon
J Korean Orthop Assoc. 2018;53(4):283-292. doi: 10.4055/jkoa.2018.53.4.283.
Reference
-
1. Coventry MB. Osteotomy of the upper portion of the tibia for degenerative arthritis of the knee. A preliminary report. J Bone Joint Surg Am. 1965; 47:984–990.2. Lexer E. Die gesamte Wiederherstellungschirurgie. Leipzig: Barth;1931.3. Brett AL. Operative correction of genu recurvatum. J Bone Joint Surg Am. 1935; 17:984–989.4. Debeyre J, Patte D. The place of corrective osteotomies in the treatment of gonarthrosis. Acta Orthop Belg. 1961; 27:374–383.5. Lee DH, Han SB, Oh KJ, et al. The weight-bearing scanogram technique provides better coronal limb alignment than the navigation technique in open high tibial osteotomy. Knee. Published online October 5, 2012; doi: 10.1016/J.Knee.2012.09.003.6. Sim JA, Kwak JH, Yang SH, Choi ES, Lee BK. Effect of weight-bearing on the alignment after open wedge high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2010; 18:874–878.7. Bonnin M, Chambat P. Current status of valgus angle, tibial head closing wedge osteotomy in media gonarthrosis. Orthopade. 2004; 33:135–142.8. Benzakour T, Hefti A, Lemseffer M, El Ahmadi JD, Bouyarmane H, Benzakour A. High tibial osteotomy for medial osteoarthritis of the knee: 15 years follow-up. Int Orthop. 2010; 34:209–215.9. Lee DH, Nha KW, Park SJ, Han SB. Preoperative and postoperative comparisons of navigation and radiologic limb alignment measurements after high tibial osteotomy. Arthroscopy. 2012; 28:1842–1850.10. Gaasbeek RD, Sonneveld H, van Heerwaarden RJ, Jacobs WC, Wymenga AB. Distal tuberosity osteotomy in open wedge high tibial osteotomy can prevent patella infera: a new technique. Knee. 2004; 11:457–461.11. Stoffel K, Willers C, Korshid O, Kuster M. Patellofemoral contact pressure following high tibial osteotomy: a cadaveric study. Knee Surg Sports Traumatol Arthrosc. 2007; 15:1094–1100.12. Lobenhoffer P, Galla M, Agneskirchner JD. Osteotomies around the knee: indications, planning, surgical techniques using plate fixators. Davos, Stuttgart, New York: AO Publishing;2008.13. Coventry MB. Upper tibial osteotomy for osteoarthritis. J Bone Joint Surg Am. 1985; 67:1136–1140.14. Hernigou P, Medevielle D, Debeyre J, Goutallier D. Proximal tibial osteotomy for osteoarthritis with varus deformity. A ten to thirteen-year follow-up study. J Bone Joint Surg Am. 1987; 69:332–354.15. Pape D, Seil R, Adam F, Rupp S, Kohn D, Lobenhoffer P. Imaging and preoperative planning of osteotomy of tibial head osteotomy. Orthopade. 2004; 33:122–134.16. Fujisawa Y, Masuhara K, Shiomi S. The effect of high tibial osteotomy on osteoarthritis of the knee. An arthroscopic study of 54 knee joints. Orthop Clin North Am. 1979; 10:585–608.17. Miniaci A, Ballmer FT, Ballmer PM, Jakob RP. Proximal tibial osteotomy. A new fixation device. Clin Orthop Relat Res. 1989; (246):250–259.18. Dugdale TW, Noyes FR, Styer D. Preoperative planning for high tibial osteotomy. The effect of lateral tibiofemoral separation and tibiofemoral length. Clin Orthop Relat Res. 1992; (274):248–264.19. Giffin JR, Vogrin TM, Zantop T, Woo SL, Harner CD. Effects of increasing tibial slope on the biomechanics of the knee. Am J Sports Med. 2004; 32:376–382.20. Flecher X, Parratte S, Aubaniac JM, Argenson JN. A 12-28-year followup study of closing wedge high tibial osteotomy. Clin Orthop Relat Res. 2006; 452:91–96.21. Han SB, Lee DH, Shetty GM, Chae DJ, Song JG, Nha KW. A "safe zone" in medial open-wedge high tibia osteotomy to prevent lateral cortex fracture. Knee Surg Sports Traumatol Arthrosc. 2013; 21:90–95.22. Brosset T, Pasquier G, Migaud H, Gougeon F. Opening wedge high tibial osteotomy performed without filling the defect but with locking plate fixation (TomoFix™) and early weight-bearing: prospective evaluation of bone union, precision and maintenance of correction in 51 cases. Orthop Traumatol Surg Res. 2011; 97:705–711.23. Shenoy PM, Oh HK, Choi JY, et al. Pseudoaneurysm of the popliteal artery complicating medial opening wedge high tibial osteotomy. Orthopedics. 2009; 32:442.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Opening Wedge High Tibia Osteotomy
- Distal Femoral Medial Opening Wedge Osteotomy for Post-Traumatic, Distal Femoral Varus Deformity
- Delayed Onset of the Popliteal Artery Pseudoaneurysm Following Medial Opening Wedge High Tibial Osteotomy
- High Tibial Osteotomy
- Severe Genu Recurvatum after a Closing-wedge High Tibial Osteotomy: A Case Report
