Ultrasonography of the Acute Abdomen
- Affiliations
-
- 1Department of Radiology, Sungkyunkwan University School of Medicine, Korea. jhlim@smc.samsung.co.kr, sjlee@smc.samsung.co.kr.
- KMID: 2184797
- DOI: http://doi.org/10.5124/jkma.2007.50.1.73
Abstract
- The initial radiologic evaluation of a patient with acute abdominal symptoms begins with plain abdominal radiographs. Plain abdominal radiographs are helpful for the diagnosis of intestinal obstruction and pneumoperitoneum. However, cross-sectional imaging modalities, such as ultrasonography or computed tomography, are necessary for specific diagnosis of acute abdomen. Ultrasonography is a non-invasive and comfortable tool for patients visiting emergency room. This article describes the ultrasonographic findings of most common diseases presenting with acute abdominal symptoms.
MeSH Terms
Figure
-
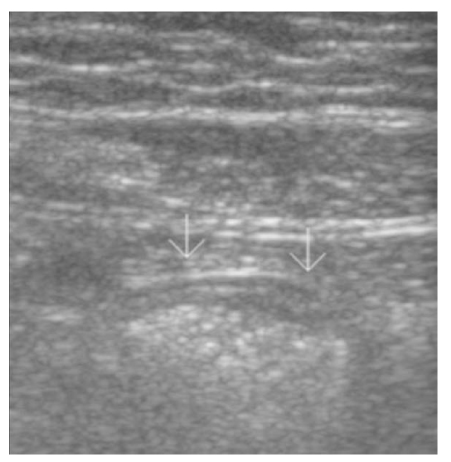
Figure 1 Normal appendix. Ultrasonogram using high frequency transducer on RLQ shows thin-walled, collapsed appendix (white arrows)
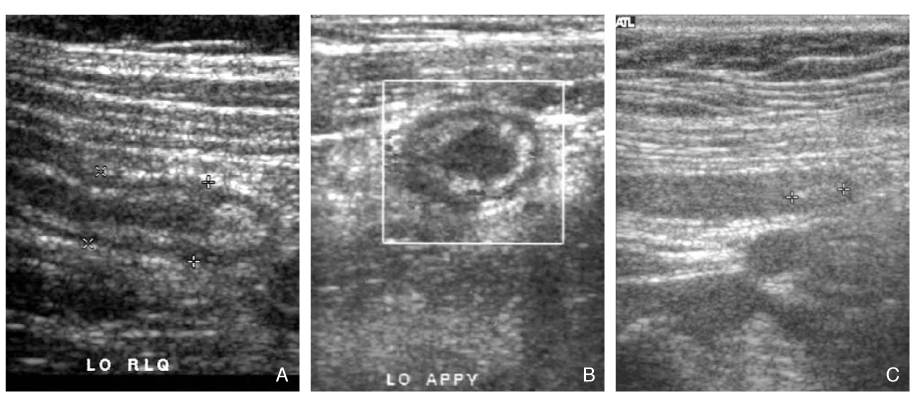
Figure 2 (A) Appendicitis. Longitudinal scan of ultrasonogram on RLQ shows thick-walled, distended appendix (diameter>6mm) (B) Color Doppler ultrasonogram shows increase blood flow in inflamed appendix (C) There is appendicolith in the tip of appendix on ultrasonogram
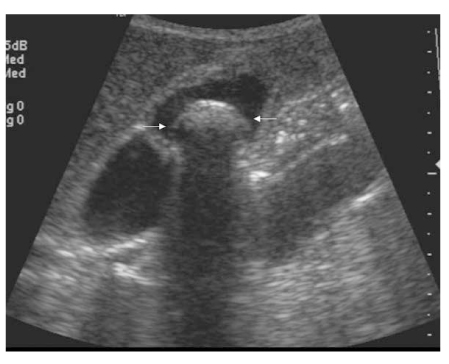
Figure 3 Acute cholecystitis. Longitudinal scan of RUQ shows large gallstone (white arrows) with wall thickening of gallbladder
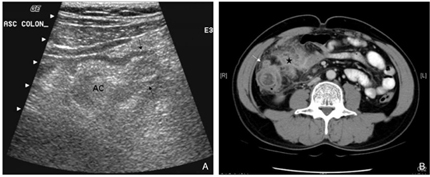
Figure 4 Diverticulitis in the ascending colon. Ultrasonogram using high frequency transducer (A) shows thickened wall of ascending colon (AC) and out-pouching sac with wall thickening (arrows). Computed tomography of lower abdomen (B) shows inflamed diverticulum (white arrow) and mesenteric infiltration (starlet)
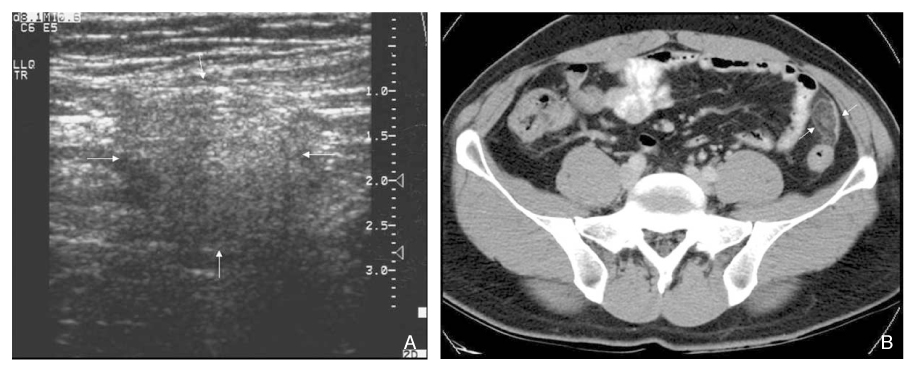
Figure 5 Appendagitis in the descending colon. Ultrasonogram in LLQ (A) shows well circumscribed echogenic mass with thin low echoic rim (white arrows) adjacent to descending colon. CT scan shows oval fatty mass (white arrows) with thin rim and internal high attenuation attached anterior wall of descending colon (B)

Figure 6 Gallstone ileus (A) Ultrasonogram of lower abdomen shows large curvilinear bright echo (white arrows) with posterior echo shadowing in dilated small intestine (B) This bright echo reveals to be stone (white arrows) on CT (C) Ultrasonogram on RUQ shows collapse of GB and bright echoes in the lumen of gallbladder indicating airs (arrows)
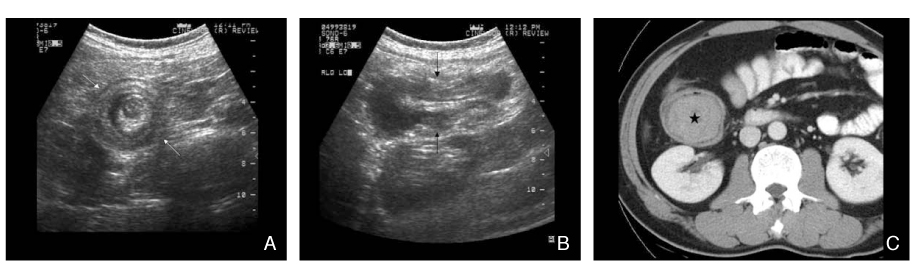
Figure 7 Intussusception of small intestine. Transverse (A) and longitudinal (B) ultrasonograms of lower abdomen show multiple layered wall of small intestine with low echogic leading mass. CT scan (C) shows homogeneous enhancing mass (starlet) at the end of the intussusceptum, revealed to be B-cell lymphoma of small intestine
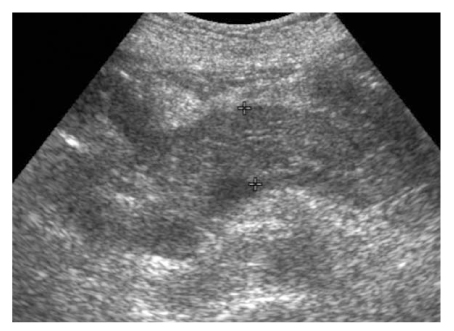
Figure 8 Acute pancreatitis. Transverse ultrasonogram on upper abdomen shows diffuse enlargement and decrease echogenecity of pancreas

Figure 9 Stone in common bile duct. Oblique longitudinal ultrasonogram shows oval echogenic lesion with acoustic shadowing (white arrows) and dilatation of extrahepatic bile duct
Cited by 1 articles
-
Usefulness of Ultrasonographic Examination by a Pediatrician in Children with Abdominal Pain
Hyun Seok Park, Ju Hee We, Jae Hong Park
Korean J Pediatr Gastroenterol Nutr. 2011;14(2):141-147. doi: 10.5223/kjpgn.2011.14.2.141.
Reference
-
1. Davies AH, Mastorakou I, Cobb R, Rogers C, Lindsell D, Mortensen NJM. Ultrasonography in the acute abdomen. Br J Surg. 1991. 78:1178–1180.
Article2. Laing FC. Ultrasonography of the acute abedomen. Radiol Clin North Am. 1992. 30:389–404.3. Heller MB, Verdile VP. Ultrasonography in emergency medicine. Emerg Med Clin North Am. 1992. 10:27–46.
Article4. Hudson PA, Promes SB. Abdominal ultrasonography. Emerg Med Clin North Am. 1997. 15:825–848.
Article5. Cosgrove D, Meire H, Dewbury K. Abdominal and general ultrasound. 1994. 1st ed. Churchill Livingstone.6. Lim JH, Kim PN, et al. Abdominal Radiology. 2005. 1st ed. Seoul: Korean Society of Abdominal Radiology.7. O'Malley M, Wilson SR. US of gastrointestinal tract abnormalities with CT correlation. Radiographics. 2003. 23:59–72.8. Vijayaraghavan SB. High-resolution sonographic spectrum of diverticulosis, diverticulitis, and their complications. J Ultrasound Med. 2006. 25:75–85.
Article9. Baker JA, Mandavia D, Swadron SP. Diagnosis of diverticulitis by bedside ultrasound in the emergency department. J Emerg Med. 2006. 30:327–329.
Article10. Singh AK, Gervais DA, Hahn P, Sagar P, Mueller PR, Novelline RA. Acute epiploic appendatitis and its mimics. Radiographics. 2005. 25:1521–1534.11. Hollerweger A, Macheiner P, Rettenbacher T, Gritzmann N. Primary epiploic appendagitis: sonographic findings with CT correlation. Journal Clinical Ultrasound. 2002. 30:481–495.
Article12. Buljevac M, Busic Z, Cabrijan Z. Sonographic diagnosis of gallstone ileus. J Ultrasound Med. 2004. 23:1395–1398.
Article13. Lassandro F, Gagliardi N, Scuderi M, Pinto A, Gatta G, Mazzeo R. Gallstone ileus analysis of radiological findings in 27 patients. Eur J Radiol. 2004. 50:23–29.
Article14. Zubaidi A, Al-Saif F, Silverman R. Adult intussusception: A retrospective review. Dis Colon Rectum. 2006. 49:1–6.
Article15. Mateen MA, Saleem S, Rao PC, Gangadhar V, Reddy DN. Transient small bowel intussusception: ultrasound findings and clinical significance. Abdom Imaging. 2006. 30:1–7.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Emergency Ultrasonography in Acute Abdomen
- Imaging Findings of Gastrointestinal Emergency in Infants and Young Children
- Clinical review on surgical acute abdomen
- Ultrasonographic Evaluation of Acute Appendicitis Superimposed on the Non-rotational Anomaly of the Gastrointestinal Tract
- Sonography of the Pediatric Acute Abdomen in the Emergency Center
