Failure of Removal of Stripped Locking Screw after Locking Compression Plating
- Affiliations
-
- 1Department of Orthopedic Surgery, School of Medicine, Keimyung University, Daegu, Korea. oslee@dsmc.or.kr
- 2Department of Emergency, School of Medicine, Keimyung University, Daegu, Korea.
- KMID: 2183860
- DOI: http://doi.org/10.12671/jkfs.2011.24.2.169
Abstract
- PURPOSE
The purpose of this study was to evaluate the incidence and possible causes of stripped locking screws that make difficult to remove the locking compression plate. We also tried to find the useful methods to remove the stripped locking screws.
MATERIALS AND METHODS
Between May 2005 and January 2009, 84 patients who underwent operations for removal of locking compression plate were included in this study. We removed 298 3.5-mm locking screws and 289 5.0-mm locking screws in these patients. We retrospectively investigated the incidence and possible causes of stripped locking screws and evaluated the pros and cons of the methods that we have used to remove the stripped locking screws.
RESULTS
17 out of 298 3.5-mm locking screws (5.7%) and 2 out of 289 5.0-mm locking screws (0.7%) were encountered with difficulties by hexagonal driver during removal because of the stripping of the hexagonal recess. First we used the conical extraction screw for all the stripped locking screws and only 3 screws were removed successfully. We removed 3 screws by cutting the plate around the stripped locking screw and twisting the plate with the screw and we removed 1 screw by the use of hallow reamer after cutting the plate. Twelve screw shafts were left except grinding of screw head by metal-cutting burr. There was one iatrogenic re-fracture in whom we have used with hallow reamer.
CONCLUSION
At the time of locking compression plate removal, difficulties of locking screw removal due to the stripping of the hexagonal recess should be expected and surgeon must prepare several methods to solve this problem.
MeSH Terms
Figure
-

Fig. 1 The conical extraction screw can be used for the removal of stripped locking screws at the first attempt.
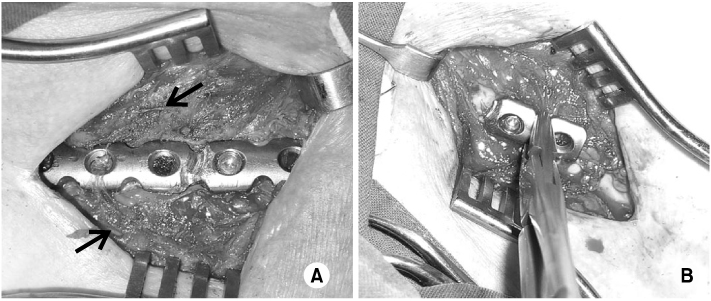
Fig. 2 (A) and (B) Stripped locking screws can be removed by cutting the plate around the screw and twisting the plate with the screw. There are a lot of metal particles around the plate (black arrows).
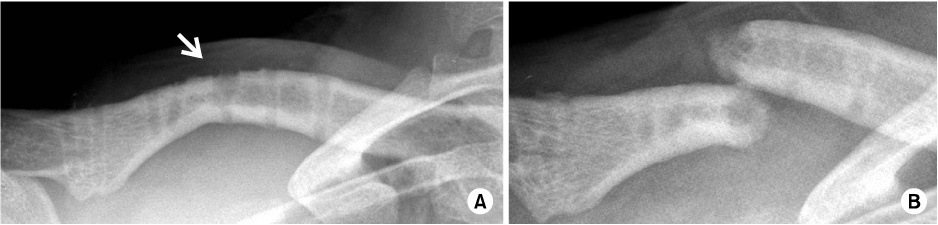
Fig. 3 (A) Stripped locking screw was removed with the hallow reamer in patient who is 21-years old male. There is cortical defect where hallow reamer was used (white arrow). (B) After one month after plate removal, re-fracture was developed without trauma.
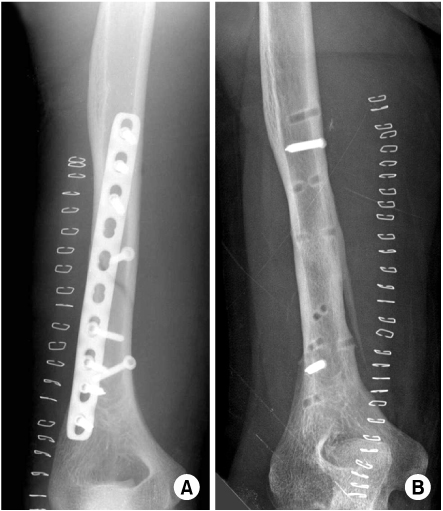
Fig. 4 (A) 29-years old male who had distal humerus fracture was treated with small locking compression plate. (B) After 24 months after initial operation, the plate was removed. There shows two remained locking screw shaft because of stripped locking screw head.

Fig. 5 (A) and (B) The targeting device can be locked in locking compression plate with wrong angle and it can causes wrong insertion angle of locking screws.
Reference
-
1. Bae JH, Oh JK, Oh CW, Hur CR. Technical difficulties of removal of locking screw after locking compression plating. Arch Orthop Trauma Surg. 2009. 129:91–95.
Article2. Cole PA, Zlowodzki M, Kregor PJ. Less Invasive Stabilization System (LISS) for fractures of the proximal tibia: indications, surgical technique and preliminary results of the UMC Clinical Trial. Injury. 2003. 34(Suppl 1):A16–A29.
Article3. Ehlinger M, Adam P, Simon P, Bonnomet F. Technical difficulties in hardware removal in titanium compression plates with locking screws. Orthop Traumatol Surg Res. 2009. 95:373–376.
Article4. Farouk O, Krettek C, Miclau T, Schandelmaier P, Guy P, Tscherne H. Minimally invasive plate osteosynthesis and vascularity: preliminary results of a cadaver injection study. Injury. 1997. 28(Suppl 1):A7–A12.
Article5. Frigg R. Development of the locking compression plate. Injury. 2003. 34(Suppl 2):B6–B10.
Article6. Frigg R. Locking compression Plate (LCP). An osteosynthesis plate based on the Dynamic Compression Plate and the Point Contact Fixator (PC-Fix). Injury. 2001. 32(Suppl 2):63–66.
Article7. Gautier E, Sommer C. Guidelines for the clinical application of the LCP. Injury. 2003. 34(Suppl 2):B63–B76.
Article8. Georgiadis GM, Gove NK, Smith AD, Rodway IP. Removal of the less invasive stabilization system. J Orthop Trauma. 2004. 18:562–564.
Article9. Hamilton P, Doig S, Williamson O. Technical difficulty of metal removal after LISS plating. Injury. 2004. 35:626–628.
Article10. Kääb MJ, Frenk A, Schmeling A, Schaser K, Schütz M, Haas NP. Locked internal fixator: sensitivity of screw/plate stability to the correct insertion angle of the screw. J Orthop Trauma. 2004. 18:483–487.11. Korner J, Lill H, Müller LP, Rommens PM, Schneider E, Linke B. The LCP-concept in the operative treatment of distal humerus fractures--biological, biomechanical and surgical aspects. Injury. 2003. 34(Suppl 2):B20–B30.12. Kregor PJ, Stannard JA, Zlowodzki M, Cole PA. Treatment of distal femur fractures using the less invasive stabilization system: surgical experience and early clinical results in 103 fractures. J Orthop Trauma. 2004. 18:509–520.
Article13. Perren SM. Evolution and rationale of locked internal fixator technology. Introductory remarks. Injury. 2001. 32(Suppl 2):B3–B9.14. Schütz M, Kääb MJ, Haas N. Stabilization of proximal tibial fractures with the LIS-System: early clinical experience in Berlin. Injury. 2003. 34(Suppl 1):A30–A35.
Article15. Suzuki T, Smith WR, Stahel PF, Morgan SJ, Baron AJ, Hak DJ. Technical problems and complications in the removal of the less invasive stabilization system. J Orthop Trauma. 2010. 24:369–373.
Article16. Wagner M. General principles for the clinical use of the LCP. Injury. 2003. 34(Suppl 2):B31–B42.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Stripping of the Hexagonal Recess in the Process of LCP (Locking Compression Plate) Removal
- Comparision of Non-locking Monocortical and Bicortical Screw System for Anterior Cervical Fusion and Plating in Degenerative Cervical Spondylosis
- Relationship between the Length of Distal Locking Screws and Diaphyseal Screws in Volar Plate Fixation of Distal Radius Fractures
- Ulnar Nerve Injury Caused by the Incomplete Insertion of a Screw Head after Internal Fixation with Dual Locking Plates in AO/OTA Type C2 Distal Humerus Fractures
- Failure of Distal Locking Screws in an Intraarticular Distal Radius Fracture Treated with Volar Locking Plate Fixation
