Outcomes and Analysis of Factors Affecting Bone Union after Interlocking Intramedullary Nailing in Segmental Tibia Fractures
- Affiliations
-
- 1Department of Orthopaedic Surgery, School of Medicine, Chosun University, Gwangju, Korea. leejy88@chosun.ac.kr
- KMID: 2183828
- DOI: http://doi.org/10.12671/jkfs.2013.26.4.275
Abstract
- PURPOSE
To evaluate the radiological results and complications of interlocking intramedullary nailing for segmental tibia fractures.
MATERIALS AND METHODS
Twenty-six patients (26 cases) who underwent interlocking intramedullary nailing for segmental tibia fractures between January 2003 and May 2011 were followed for more than one year. We evaluated the complications and statistically analyzed the factors influencing bone union, including open fracture, fracture site, reaming, postoperative angulation, and postoperative fracture gap.
RESULTS
Nineteen cases (73%) achieved bone union with one operation at an average of 7 months (range, 5 to 11). Seven cases had secondary procedures before achieving union. Complications included 7 cases of nonunion, 3 cases of incomplete peroneal nerve injury, 2 cases of superficial infection, 1 case of compartment syndrome. Factors showing statistically significant differences were open fracture, postoperative angulation, and postoperative fracture gap. Factors showing no statistically significant difference were fracture site and reaming.
CONCLUSION
Nonunion is the most common complication in interlocking intramedullary nailing for segmental tibia fractures. To minimize this complication, comprehension of surgical techniques to reduce anatomically and careful evaluation of the fracture are required.
Keyword
MeSH Terms
Figure
-

Fig. 1 (A, B) Preoperative radiographs of a 56-year-old man show a tibia segmental fracture classified as AO/OTA type 43-C2. (C, D) The segmental tibia fracture was stabilized with intramedullary interlocking nailing using reaming. (E, F) Postoperative radiographs show complete bone union with good alignment at 14 months after surgery.
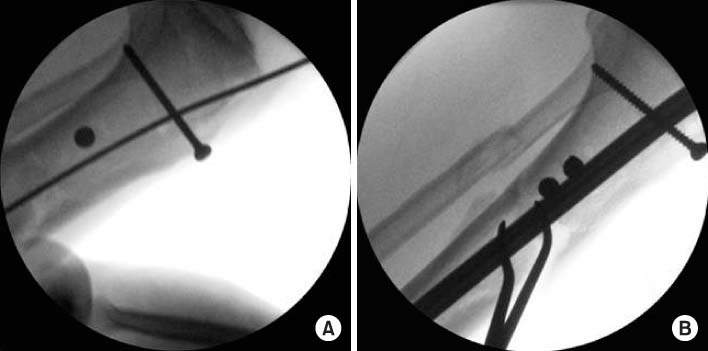
Fig. 2 (A) Intraoperative C-arm image using the blocking screw technique in the proximal portion of segmental tibia fracture. (B) Intraoperative C-arm image shows good alignment and reduction after intramedullary nailing with a blocking screw on the tibia proximal portion.

Fig. 3 (A, B) Preoperative radiographs of a 47-year-old man show a tibia segmental fracture classified as AO/OTA type 43-C2. (C, D) Postoperative radiographs show good alignment and reduction after intramedullary interlocking nailing with additional plating on the tibia proximal portion.

Fig. 4 (A, B) Preoperative radiographs of a 51-year-old man show a tibia segmental open fracture classified as AO/OTA type 43-C2. (C, D) Initial clinical photo shows Gustilo-Anderson classification IIIA open wound, exposing the bone and muscle. (E, F) Segmental tibia fracture was stabilized with intramedullary interlocking nailing using unreaming. (G, H) Follow up x-ray at 16 months after surgery shows nonunion in the proximal and distal sites. (I) Reoperation has been done with exchange nailing. Postoperative radiographs show complete bone union at 28 months after primary surgery.
Reference
-
1. Bone LB, Kassman S, Stegemann P, France J. Prospective study of union rate of open tibial fractures treated with locked, unreamed intramedullary nails. J Orthop Trauma. 1994; 8:45–49.
Article2. Borrelli J Jr, Prickett W, Song E, Becker D, Ricci W. Extraosseous blood supply of the tibia and the effects of different plating techniques: a human cadaveric study. J Orthop Trauma. 2002; 16:691–695.
Article3. Canale ST, Beaty JH. Campbell's operative orthopaedics. 11th ed. Philadelphia: Mosby;2008. vol. 3:p. 3530.4. Catagni MA, Guerreschi F, Holman JA, Cattaneo R. Distraction osteogenesis in the treatment of stiff hypertrophic nonunions using the Ilizarov apparatus. Clin Orthop Relat Res. 1994; 301:159–163.
Article5. Chun CH, Lee BC, Hwang GT, Kwon SG, Lee HS. Tibial segmental fracture treated with interlocking intramedullary nail. J Korean Soc Fract. 1997; 10:534–540.
Article6. Collinge CA, Sanders RW. Percutaneous plating in the lower extremity. J Am Acad Orthop Surg. 2000; 8:211–216.
Article7. Fisher WD, Hamblen DL. Problems and pitfalls of compression fixation of long bone fractures: a review of results and complications. Injury. 1978; 10:99–107.
Article8. Huang CK, Chen WM, Chen TH, Lo WH. Segmental tibial fractures treated with interlocking nails. A retrospective study of 33 cases. Acta Orthop Scand. 1997; 68:563–566.
Article9. Hupel TM, Weinberg JA, Aksenov SA, Schemitsch EH. Effect of unreamed, limited reamed, and standard reamed intramedullary nailing on cortical bone porosity and new bone formation. J Orthop Trauma. 2001; 15:18–27.
Article10. Krettek C, Miclau T, Schandelmaier P, Stephan C, Mohlmann U, Tscherne H. The mechanical effect of blocking screws ("Poller screws") in stabilizing tibia fractures with short proximal or distal fragments after insertion of small-diameter intramedullary nails. J Orthop Trauma. 1999; 13:550–553.
Article11. Lang GJ, Cohen BE, Bosse MJ, Kellam JF. Proximal third tibial shaft fractures. Should they be nailed? Clin Orthop Relat Res. 1995; (315):64–74.12. Langard O, Bo O. Segmental tibial shaft fractures. Acta Orthop Scand. 1976; 47:351–357.
Article13. Leunig M, Hertel R. Thermal necrosis after tibial reaming for intramedullary nail fixation. A report of three cases. J Bone Joint Surg Br. 1996; 78:584–587.14. Melis GC, Sotgiu F, Lepori M, Guido P. Intramedullary nailing in segmental tibial fractures. J Bone Joint Surg Am. 1981; 63:1310–1318.
Article15. Nicoll EA. Fractures of the tibial shaft. A survey of 705 cases. J Bone Joint Surg Br. 1964; 46:373–387.16. Olerud S, Karlstrom G. Tibial fractures treated by AO compression osteosynthesis. Experiences from a five year material. Acta Orthop Scand Suppl. 1972; 140:1–104.
Article17. Rhee JH, Lee JW, Cho JY, Bae SW, Yoon SH, Lee JY. Nonunion after interlocking intramedullay nailing in tibia segmental fractures. J Korean Soc Fract. 1997; 10:309–315.
Article18. Robinson CM, McLauchlan GJ, McLean IP, Court-Brown CM. Distal metaphyseal fractures of the tibia with minimal involvement of the ankle. Classification and treatment by locked intramedullary nailing. J Bone Joint Surg Br. 1995; 77:781–787.
Article19. Song GH. Treatment of femoral fractures by bone grafting from trochanter and interlocking intramedullary nail fixation. Zhongguo Gu Shang. 2010; 23:950–951.20. Song KJ, Lee KB, Hwang BY. Analysis for the factors influencing bone union in segmental tibial shaft fractures treated with interlocking intramedullary nailing. J Korean Fract Soc. 2004; 17:153–159.
Article21. Tarr RR, Resnick CT, Wagner KS, Sarmiento A. Changes in tibiotalar joint contact areas following experimentally induced tibial angular deformities. Clin Orthop Relat Res. 1985; (199):72–80.
Article22. Tornetta P 3rd, Collins E. Semiextended position of intramedullary nailing of the proximal tibia. Clin Orthop Relat Res. 1996; (328):185–189.23. Tucker HL, Kendra JC, Kinnebrew TE. Management of unstable open and closed tibial fractures using the Ilizarov method. Clin Orthop Relat Res. 1992; (280):125–135.
Article24. Wu CC, Shih CH. Segmental tibial shaft fractures treated with interlocking nailing. J Orthop Trauma. 1993; 7:468–472.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment of Tibial Fractures by Interlocking Intramedullary Nailling
- Interlocking Intramedullary Nailing in the Treatment of the Tibial Shaft Fractures: Comparative Study between Reamed and Unreamed Nailing
- Interlocking Nailing in Segmental Tibial Fractures: The Problems of the Fractures involving Proximal Portion
- Interlocking Intramedullary Nailing for the Treatment of Segmental Fractures of the Femur
- Interlocking Intramedullary Nailing Versus conventional Kuntscher Intramedullary Nailing for Fracture of the Femoral Shaft
