Clinical Results of Excision of Hamate Hook in the Baseball Players with Hamate Hook Nonunion
- Affiliations
-
- 1Department of Orthopaedic Surgery, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea. lsjmd@naver.com
- KMID: 2183759
- DOI: http://doi.org/10.12671/jkfs.2016.29.1.12
Abstract
- PURPOSE
The purpose of this study is to report the clinical results of excision of the hamate hook in baseball players with hamate hook nonunion.
MATERIALS AND METHODS
This study included 10 baseball players treated with excision of the hamate hook. Among 10 players, there were 3 professional players and 7 amateur players. The clinical outcomes were evaluated using the visual analog scale (VAS) pain score, exercise performance score, and grip power. We also checked complications and time to return to the game.
RESULTS
At final follow-up, the average VAS score was 0.4 points and the average performance score was 9.0 points. The grip power was recovered to 96.7% of the opposite hand at final follow-up. Significant improvement in pain and grip power was observed after surgery. The average time to return to the game was 11.8 weeks. There was one case of postoperative ulnar nerve neuropathy, which was completely resolved within 12 weeks after surgery.
CONCLUSION
We think that excision of the hamate hook is an effective treatment to enable early return to the game without loss of grip strength in the baseball player with nonunion of the hamate hook.
Keyword
Figure
-
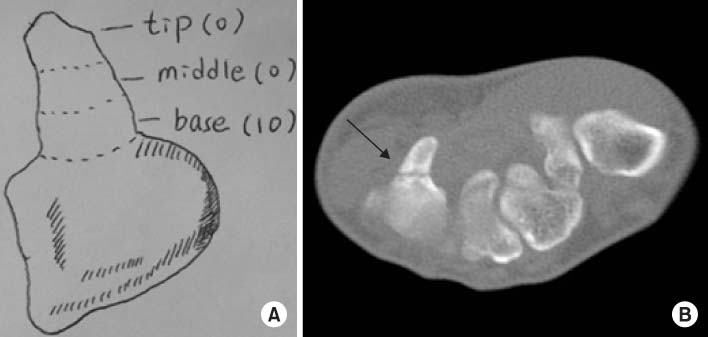
Fig. 1 (A) Classification of hamate hook fractures. Number in parenthesis indicates number of patients. (B) Computed tomography-axial view shows nonunion of a hamate hook fracture (arrow).
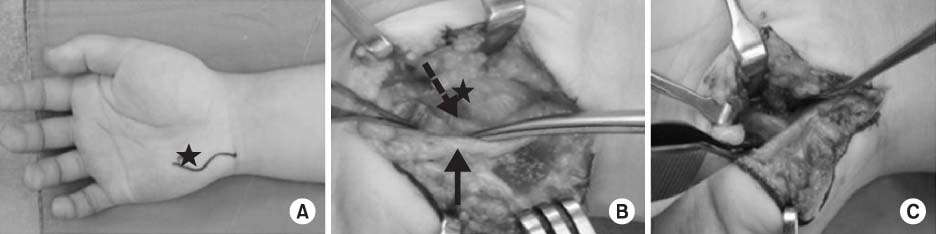
Fig. 2 (A) A curved skin incision was made on the hypothenar eminence (asterisk: hamate hook). (B) After careful retraction of the superficial branch of the ulnar nerve (dashed arrow) ulnarly, the hamate hook (asterisk) and the deep branch of the ulnar nerve (arrow) can be found. (C) The hamate hook was removed carefully.
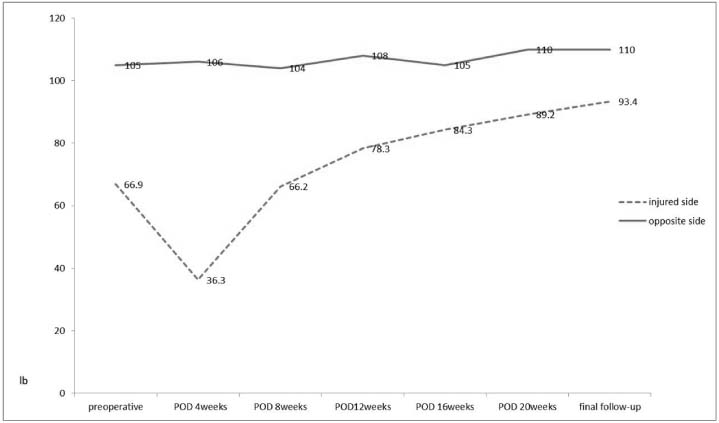
Fig. 3 The grip power was recovered to 96.7% of the opposite hand at the final follow-up. POD: Postoperative day.

Fig. 4 Location of the hamate hook relative to a bat end in the nondominant right hand of a left-handed hitter. H: Hamate hook, P: Pisform.
Reference
-
1. Boulas HJ, Milek MA. Hook of the hamate fractures. Diagnosis, treatment, and complications. Orthop Rev. 1990; 19:518–529.2. O'Shea K, Weiland AJ. Fractures of the hamate and pisiform bones. Hand Clin. 2012; 28:287–300.3. Bishop AT, Beckenbaugh RD. Fracture of the hamate hook. J Hand Surg Am. 1988; 13:135–139.
Article4. Demirkan F, Calandruccio JH, Diangelo D. Biomechanical evaluation of flexor tendon function after hamate hook excision. J Hand Surg Am. 2003; 28:138–143.
Article5. Watson HK, Rogers WD. Nonunion of the hook of the hamate: an argument for bone grafting the nonunion. J Hand Surg Am. 1989; 14:486–490.
Article6. Nanno M, Sawaizumi T, Ito H. Simplified dorsal approach to fracture of the hamate hook with percutaneous fixation with screws. J Plast Surg Hand Surg. 2010; 44:214–218.
Article7. Carter PR, Eaton RG, Littler JW. Ununited fracture of the hook of the hamate. J Bone Joint Surg Am. 1977; 59:583–588.
Article8. Futami T, Aoki H, Tsukamoto Y. Fractures of the hook of the hamate in athletes. 8 cases followed for 6 years. Acta Orthop Scand. 1993; 64:469–471.
Article9. Stark HH, Jobe FW, Boyes JH, Ashworth CR. Fracture of the hook of the hamate in athletes. J Bone Joint Surg Am. 1977; 59:575–582.
Article10. Wright TW, Moser MW, Sahajpal DT. Hook of hamate pull test. J Hand Surg Am. 2010; 35:1887–1889.
Article11. Stark HH, Chao EK, Zemel NP, Rickard TA, Ashworth CR. Fracture of the hook of the hamate. J Bone Joint Surg Am. 1989; 71:1202–1207.
Article12. Devers BN, Douglas KC, Naik RD, Lee DH, Watson JT, Weikert DR. Outcomes of hook of hamate fracture excision in high-level amateur athletes. J Hand Surg Am. 2013; 38:72–76.
Article13. Rettig AC. Athletic injuries of the wrist and hand. Part I: traumatic injuries of the wrist. Am J Sports Med. 2003; 31:1038–1048.14. Walsh JJ 4th, Bishop AT. Diagnosis and management of hamate hook fractures. Hand Clin. 2000; 397–403. viii
Article15. Parker RD, Berkowitz MS, Brahms MA, Bohl WR. Hook of the hamate fractures in athletes. Am J Sports Med. 1986; 14:517–523.
Article16. Andresen R, Radmer S, Sparmann M, Bogusch G, Banzer D. Imaging of hamate bone fractures in conventional X-rays and high-resolution computed tomography. An in vitro study. Invest Radiol. 1999; 34:46–50.
Article17. Marchessault J, Conti M, Baratz ME. Carpal fractures in athletes excluding the scaphoid. Hand Clin. 2009; 25:371–388.
Article18. Scheufler O, Andresen R, Radmer S, Erdmann D, Exner K, Germann G. Hook of hamate fractures: critical evaluation of different therapeutic procedures. Plast Reconstr Surg. 2005; 115:488–497.
Article19. Smith P 3rd, Wright TW, Wallace PF, Dell PC. Excision of the hook of the hamate: a retrospective survey and review of the literature. J Hand Surg Am. 1988; 13:612–615.
Article20. Tolat AR, Humphrey JA, McGovern PD, Compson J. Surgical excision of ununited hook of hamate fractures via the carpal tunnel approach. Injury. 2014; 45:1554–1556.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hamate Hook Fracture with Flexor Tendon Ruptures as a Golf Injury
- Fragment Excision for the Treatment of Hamate Hook Nonunion
- A roentgenographic study of the appearance of the hook of the hamate
- Non-union of Golf Related Fracture of the Hook of Hamate: A case report
- Internal Fixation of Hamate Hook Fracture by Dorsal Percutaneous Headless Compression Screw and Cortical Screw: A Technical Note
