Primary Gastric Malignant Melanoma Mimicking Adenocarcinoma
- Affiliations
-
- 1Department of Surgery, Korea University College of Medicine, Seoul, Korea. ppongttai@gmail.com
- 2Department of Pathology, Korea University College of Medicine, Seoul, Korea.
- KMID: 2183655
- DOI: http://doi.org/10.5230/jgc.2014.14.4.279
Abstract
- We report a case of primary gastric malignant melanoma that was diagnosed after curative resection but initially misdiagnosed as adenocarcinoma. A 68-year-old woman was referred to our department for surgery for gastric adenocarcinoma presenting as a polypoid lesion with central ulceration located in the upper body of the stomach. The preoperative diagnosis was confirmed by endoscopic biopsy. We performed laparoscopic total gastrectomy, and the final pathologic evaluation led to the diagnosis of primary gastric malignant melanoma without a primary lesion detected in the body. To the best of our knowledge, primary gastric malignant melanoma is extremely rare, and this is the first case reported in our country. According to the literature, it has aggressive biologic activity compared with adenocarcinoma, and curative resection is the only promising treatment strategy. In our case, the patient received an early diagnosis and underwent curative gastrectomy with radical lymphadenectomy, and no recurrence was noted for about two years.
Keyword
MeSH Terms
Figure
-
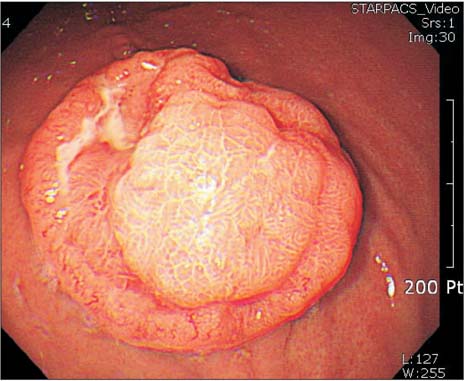
Fig. 1 Grossly, the tumor was a round, polypoid lesion with central ulceration on gastroscopy.
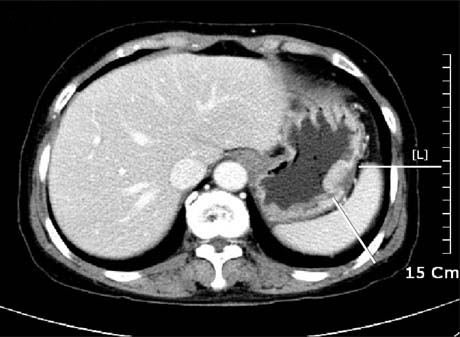
Fig. 2 Computed tomography showed a focal enhancing wall thickening in the greater curvature of the upper body of the stomach. Enlarged perigastric lymph nodes were not noted.

Fig. 3 Photograph of the gross specimen that contained a polypoid tumor with central ulceration 3 cm in diameter located in the greater curvature of the upper body of the stomach.

Fig. 4 Microscopic findings showed that tumor cells were spreading through the submucosal layer of the stomach with a clear resection margin (A: H&E, ×20; B: H&E, ×200).
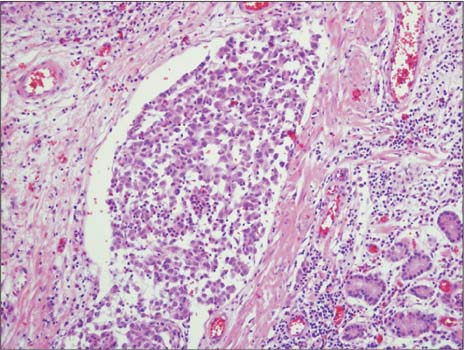
Fig. 5 Findings of immunohistochemical staining: lymphatic tumor emboli were noted by immunostaining with CD-31 and D2-40 antibody (×200).
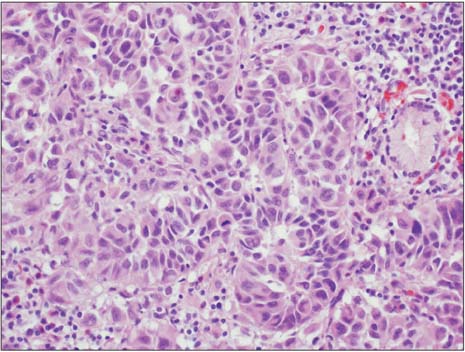
Fig. 6 The tumor cells contained atypical hyperchromatic nuclei on H&E staining (×400).

Fig. 7 The tumor nest was accompanied by melanin on H&E staining (×400).
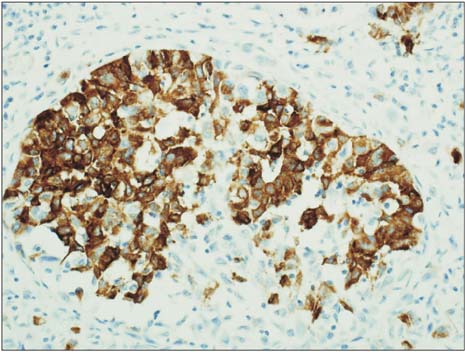
Fig. 8 Immunohistochemical examination revealed a positive reaction with HMB-45 antibodies and S-100 proteins and a negative reaction with cytokeratin antibodies (immunostaining, ×200).
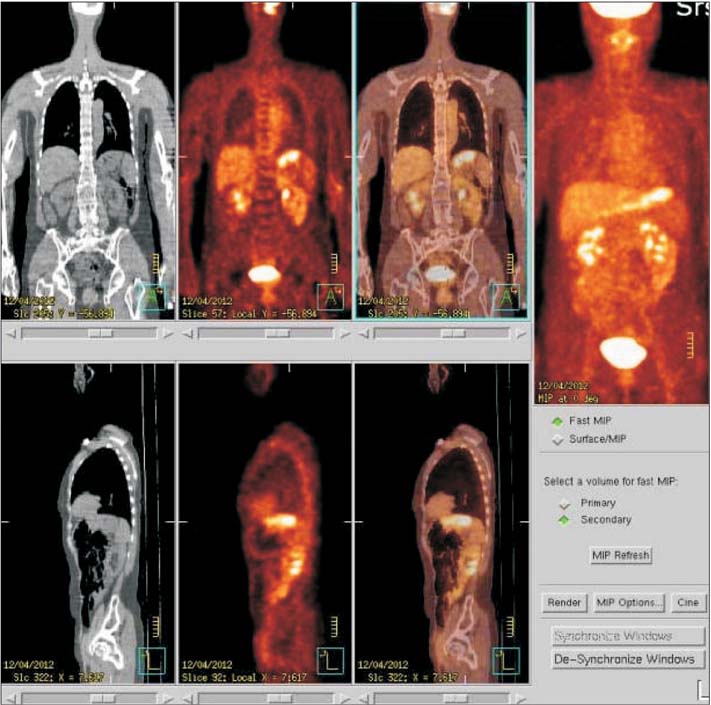
Fig. 9 Positron emission tomography/computed tomography scan showed no other hot spots except the stomach cancer portion.
Reference
-
1. Elsayed AM, Albahra M, Nzeako UC, Sobin LH. Malignant melanomas in the small intestine: a study of 103 patients. Am J Gastroenterol. 1996; 91:1001–1006.2. Woollons A, Derrick EK, Price ML, Darley CR. Gastrointestinal malignant melanoma. Int J Dermatol. 1997; 36:129–131.
Article3. Liang KV, Sanderson SO, Nowakowski GS, Arora AS. Metastatic malignant melanoma of the gastrointestinal tract. Mayo Clin Proc. 2006; 81:511–516.
Article4. Patel JK, Didolkar MS, Pickren JW, Moore RH. Metastatic pattern of malignant melanoma. A study of 216 autopsy cases. Am J Surg. 1978; 135:807–810.5. Lagoudianakis EE, Genetzakis M, Tsekouras DK, Papadima A, Kafiri G, Toutouzas K, et al. Primary gastric melanoma: a case report. World J Gastroenterol. 2006; 12:4425–4427.
Article6. Yamamura K, Kondo K, Moritani S. Primary malignant melanoma of the stomach: report of a case. Surg Today. 2012; 42:195–199.
Article7. Goral V, Ucmak F, Yildirim S, Barutcu S, Ileri S, Aslan I, et al. Malignant melanoma of the stomach presenting in a woman: a case report. J Med Case Rep. 2011; 5:94.
Article8. Alazmi WM, Nehme OS, Regalado JJ, Rogers AI. Primary gastric melanoma presenting as a nonhealing ulcer. Gastrointest Endosc. 2003; 57:431–433.
Article9. Germano D, Rosati G, Romano R, Vita G, Lepore G, De Sanctis D, et al. Primary gastric melanoma presenting as a double ulcer. J Clin Gastroenterol. 2004; 38:828.
Article10. Jelincic Z, Jakic-Razumovic J, Petrovic I, Cavcic AM, Unusic J, Trotic R. Primary malignant melanoma of the stomach. Tumori. 2005; 91:201–203.
Article11. Cheung MC, Perez EA, Molina MA, Jin X, Gutierrez JC, Franceschi D, et al. Defining the role of surgery for primary gastrointestinal tract melanoma. J Gastrointest Surg. 2008; 12:731–738.
Article12. Marsden JR, Newton-Bishop JA, Burrows L, Cook M, Corrie PG, Cox NH, et al. British Association of Dermatologists Clinical Standards Unit. Revised UK guidelines for the management of cutaneous melanoma 2010. Br J Dermatol. 2010; 163:238–256.
Article13. Krausz MM, Ariel I, Behar AJ. Primary malignant melanoma of the small intestine and the APUD cell concept. J Surg Oncol. 1978; 10:283–288.
Article14. Verma S, Petrella T, Hamm C, Bak K, Charette M. Melanoma Disease Site Group of Cancer Care Ontario's Program in Evidence-based Care. Biochemotherapy for the treatment of metastatic malignant melanoma: a clinical practice guideline. Curr Oncol. 2008; 15:85–89.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Primary malignant melanoma arising in a cystic teratoma
- A Curious Case of Primary Gastric Mucosal Melanoma
- A Case of Primary Malignant Melanoma of the Vagina: Trial of a Wide Local Excision of Vagina and Rectum
- Primary Pulmonary Malignant Melanoma Presenting as Bilateral Multiple Subsolid Nodules: A Case Report
- Synchronous Primary Anorectal Melanoma and Sigmoid Adenocarcinoma
