J Korean Med Assoc.
2005 Jul;48(7):601-608. 10.5124/jkma.2005.48.7.601.
Surgical Correction of Hyperopia
- Affiliations
-
- 1Department of Ophthalomology, Sungkyunkwan University School of Medicine, Samsung Medical Center, Korea. eschung@smc.samsung.co.kr
- KMID: 2183584
- DOI: http://doi.org/10.5124/jkma.2005.48.7.601
Abstract
- Surgical modalities to correct hyperopia include photorefractive keratectomy (PRK), laser in situ keratomileusis (LASIK), Ho:YAG laser thermal keratoplasty (LTK), conductive keratoplasty (CK), phakic IOL, and refractive lens exchange. Excimer laser-based techniques, which include LASIK, LASEK, and PRK, are currently the most popular forms of surgery to correct not only myopia and astigmatism but also hyperopia. These techniques have been reported to be safe and effective for both primary surgeries and enhancements. However, various complications related to the flap and loss of best corrected visual acuity associated with a smaller optic zone, decentration, and irregular ablation caused by longer treatment time in high hyperopia over +5 diopter can have adverse effects on visual outcomes. The development of non-excimer laser-based techniques offers viable alternatives for laser vision correction techniques. More recent non-excimer-based thermal refractive techniques include LTK and CK. Earlier forms of thermal techniques showed a lack of predictability and stability, resulting in no further development of them. Recently, CK, a laserless, radiofrequency-based technique, has been approved by the FDA for the correction of low to moderate hyperopia even though the refractive instability has not been solved yet. In high hyperopia, lens approach like phakic IOL or refractive lens exchange instead of corneal surgery is preferred. ICL (Implantable contact lens) and Artisan is the most popular lens model that has well proven clinical results concerning its safety and effectiveness. Accommodative IOL or multifocal IOL could be the solution for pseudophakic presbyopia in refractive lens exchange in the future.
MeSH Terms
Figure
-
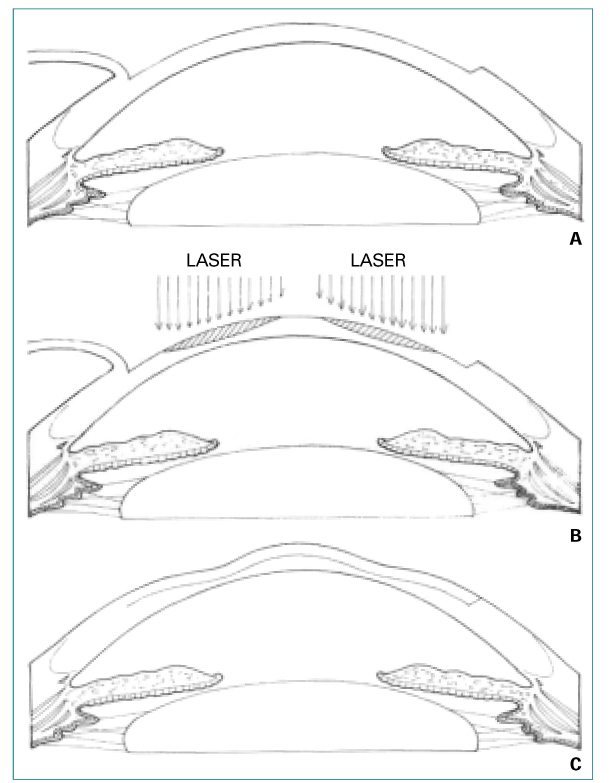
Figure 1
Figure 2
Figure 3

Figure 4
Figure 5

Figure 6
Cited by 1 articles
-
Clinical Outcomes of Toric Iris-fixated Phakic Intraocular Lens: Six-Month Follow-up
Jae Lim Chung, Sun Woong Kim, Tae-im Kim, Hyung Keun Lee, Eung Kweon Kim
J Korean Ophthalmol Soc. 2008;49(1):48-56. doi: 10.3341/jkos.2008.49.1.48.
Reference
-
1. Duke Elder S. Parson's Diseases of the Eye. 1970. 15th ed. London: Churchill;88.2. Huang B. Update on nonexcimer laser refractive surgery technique: conductive keratoplasty. Curr Opin Ophthalmol. 2003. 14:203–206.
Article4. Qazi MA, Roberts CJ, Mahmoud AM, Pepose JS. Topographic and biomechanical differences between hyperopic and myopic laser in situ keratomileusis. J Cataract Refract Surg. 2005. 31:48–60.
Article5. Zadok D, Raifkup F, Landau D, Frucht-Pery J. Long-term evaluation of hyperopic laser in situ keratomileusis. J Cataract Refract Surg. 2003. 29:2181–2188.
Article6. Autrata R, Rehurek J. laser-assisted subepithelial keratectomy and photorefractive keratectomy for the correction of hyperopia: Results of a 2-year follow-up. J Cataract Refract Surg. 2003. 29:2105–2114.
Article7. Choi RY, Wilson SE. Hyperopic laser in situ keratomileusis: primary and secondary treatments are safe and effective. Cornea. 2001. 20:388–393.8. Goker S, Er H, Kahvecioglu C. Laser in situ keratomileusis to correct hyperopia from +4.25 to +8.00 diopters. J Refract Surg. 1998. 14:26–30.
Article9. Rashad KM. Laser in situ keratomileusis for the correction of hyperopia from +1.25 to +5.00 diopters with the Technolas Keracor 117C laser. J Refract Surg. 2001. 17:113–122.
Article10. Nano HD, Muzzin S. Noncontact holmium: YAG laser thermal keratoplasty for hyperopia. J Cataract Refract Surg. 1998. 24:751–757.11. Lin D, Manche EE. Two-year results of conductive keratoplasty for the correction of low to moderate hyperopia. J Cataract Refract Surg. 2003. 29:2339–2350.
Article12. Pop M, Payette M. Refractive lens exchange versus iris-claw Artisan phakic intraocular lens for hyperopia. J Refract Surg. 2004. 20:20–24.
Article13. Davidorf JM, Zaldivar R, Oscherow S. Posterior chamber phakic intraocular lens for hyperopia of +4 to +11 diopters. J Refract Surg. 1998. 14:306–311.
Article14. Dick HB. Accommodative intraocular lenses: current status. Curr Opin Ophthalmol. 2005. 16:8–26.
Article15. Alio TL, Tavolato M, De La Hoz F, Claramonte P, Rodriguez-Pratz JL, Galal A. Near vision restoration with refractive lens exchange and pseudoaccommodating and multifocal refractive and diffractive intraocular lenses: comparative clinical study. J Cataract Refract Surg. 2004. 30:2494–2503.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Visual Outcome in Bilateral Hyperopic Amblyopia
- Surgical Results of Patients with +3.00 Diopters or More Hyperopia and Exotropia
- Clinical Features of Refractive Accommodative Esotropia According to Degree of Hypermetropia
- Comparison of Clinical Features in Hypermetropic Children According to Refractive Error
- Spontaneous Consecutive Exotropia
