J Cardiovasc Ultrasound.
2014 Jun;22(2):80-83. 10.4250/jcu.2014.22.2.80.
Pheochromocytoma as a Rare Hidden Cause of Inverted Stress Cardiomyopathy
- Affiliations
-
- 1Department of Internal Medicine, Christian Hospital, Gwangju, Korea.
- 2Department of Cardiology, Chonnam National University Hospital, Gwangju, Korea. christiankyehun@hanmail.net
- KMID: 2177463
- DOI: http://doi.org/10.4250/jcu.2014.22.2.80
Abstract
- Stress cardiomyopathy (SCMP) is characterized by a transient left ventricular dysfunction associated with apical ballooning and compensatory hyperkinesias of the basal segments after emotional or physical stress, but inverted or mid-ventricular variants of SCMP have also been described. Although catecholamine excess has been suggested as a possible pathophysiologic mechanism of SCMP, the etiology of SCMP is still unknown. Here, we report a case of inverted type of SCMP with clinical presentation mimicking acute coronary syndromes. The cause or precipitating stressor was unclear initially, but pheochromocytoma has been demonstrated as a cause of SCMP during clinical follow-up at out-patient clinic in the present case. Catecholamine-producing tumors should be included in the evaluation or management of SCMP, even though initial clinical manifestations are not suggestive for pheochromocytoma.
Keyword
MeSH Terms
Figure
-

Fig. 1 Echocardiography revealed akinesia or dyskinesia of the basal segments of the left ventricle on apical 2 chamber view (A: diastole, B: systole). Bull's eye mapping of two-dimensional speckle tracking strain imaging showed mostly positive longitudinal strain values of the basal segments and normal or increased strain values of the mid to apical segments (C).
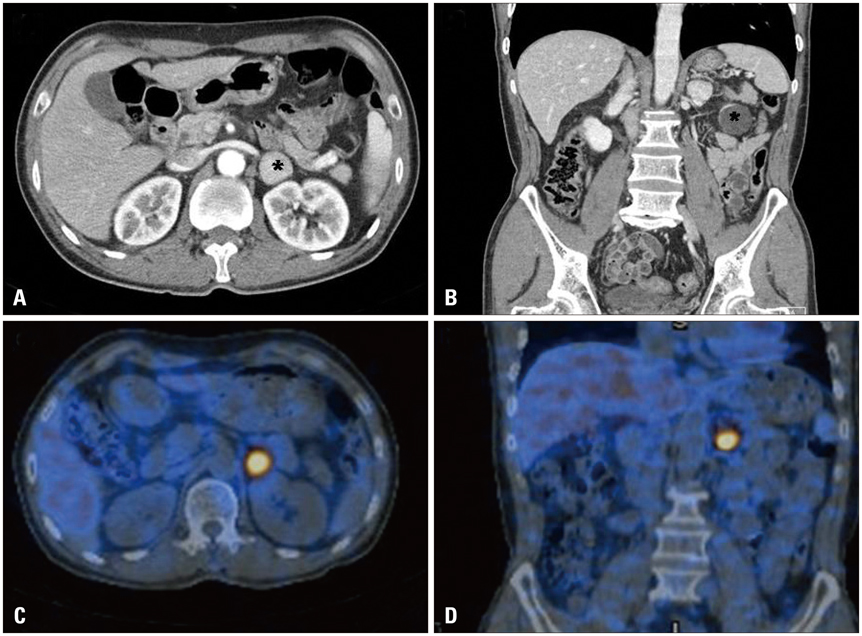
Fig. 2 A and B: Abdominal computed tomography revealed about 2.5 cm sized homogeneously enhancing well demarcated mass on left adrenal gland. Asterisk indicates left adrenal mass. C and D: I-123 metaiodobenzylguanidine (MIBG) scan revealed focal uptake of MIBG on left adrenal gland.
Reference
-
1. Tsuchihashi K, Ueshima K, Uchida T, Oh-mura N, Kimura K, Owa M, Yoshiyama M, Miyazaki S, Haze K, Ogawa H, Honda T, Hase M, Kai R, Morii I. Angina Pectoris-Myocardial Infarction Investigations in Japan. Transient left ventricular apical ballooning without coronary artery stenosis: a novel heart syndrome mimicking acute myocardial infarction. Angina Pectoris-Myocardial Infarction Investigations in Japan. J Am Coll Cardiol. 2001; 38:11–18.
Article2. Bybee KA, Prasad A. Stress-related cardiomyopathy syndromes. Circulation. 2008; 118:397–409.
Article3. Hwang SH, Kim KH, Yoon HJ, Hong YJ, Kim JH, Ahn YK, Jeong MH, Cho JG, Park JC, Kang JC. Stress cardiomyopathy complicated by left ventricular thrombi and cerebral infarctions in a patient with essential thrombocythemia. J Cardiovasc Ultrasound. 2011; 19:87–90.
Article4. Abraham J, Mudd JO, Kapur NK, Klein K, Champion HC, Wittstein IS. Stress cardiomyopathy after intravenous administration of catecholamines and beta-receptor agonists. J Am Coll Cardiol. 2009; 53:1320–1325.
Article5. Renard J, Clerici T, Licker M, Triponez F. Pheochromocytoma and abdominal paraganglioma. J Visc Surg. 2011; 148:e409–e416.
Article6. Kassim TA, Clarke DD, Mai VQ, Clyde PW, Mohamed Shakir KM. Catecholamine-induced cardiomyopathy. Endocr Pract. 2008; 14:1137–1149.
Article7. Agarwal G, Sadacharan D, Kapoor A, Batra A, Dabadghao P, Chand G, Mishra A, Agarwal A, Verma AK, Mishra SK. Cardiovascular dysfunction and catecholamine cardiomyopathy in pheochromocytoma patients and their reversal following surgical cure: results of a prospective case-control study. Surgery. 2011; 150:1202–1211.
Article8. Prejbisz A, Lenders JW, Eisenhofer G, Januszewicz A. Cardiovascular manifestations of phaeochromocytoma. J Hypertens. 2011; 29:2049–2060.
Article9. Rossi AP, Bing-You RG, Thomas LR. Recurrent takotsubo cardiomyopathy associated with pheochromocytoma. Endocr Pract. 2009; 15:560–562.
Article10. Kim S, Yu A, Filippone LA, Kolansky DM, Raina A. Inverted-Takotsubo pattern cardiomyopathy secondary to pheochromocytoma: a clinical case and literature review. Clin Cardiol. 2010; 33:200–205.
Article11. Cho DK, Kim JH, Chung N. Cardiovascular flashlight. Transient mid-ventricular ballooning cardiomyopathy associated with bladder pheochromocytoma. Eur Heart J. 2009; 30:1202.
Article12. Bybee KA, Kara T, Prasad A, Lerman A, Barsness GW, Wright RS, Rihal CS. Systematic review: transient left ventricular apical ballooning: a syndrome that mimics ST-segment elevation myocardial infarction. Ann Intern Med. 2004; 141:858–865.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of pheochromocytoma presenting as inverted Takotsubo cardiomyopathy
- A Case of Malignant Pheochromocytoma Presenting as Inverted Takotsubo-Like Cardiomyopathy
- A case of stress-induced cardiomyopathy with an "inverted Takotsubo" contractile pattern
- A Case of Pheochromocytoma That Presented as Inverted Takotsubo Cardiomyopathy
- A Case of Reversal of Takotsubo Cardiomyopathy in Patient with Pheochromocytoma
