Management of separated file in the root canal
- Affiliations
-
- 1Department of Conservative Dentistry, College of Dentistry, Kangnung National University, Korea. mendo7@kangnung.ac.kr
- 2Department of Conservative Dentistry, College of Dentistry, Wonkwang University, Korea.
- KMID: 2175815
- DOI: http://doi.org/10.5395/JKACD.2006.31.3.161
Abstract
- During root canal preparation procedures, the potential for instrument separation is always present. Files, a lentulo, a Gates-Glidden (GG) bur or any manufactured obstruction can be left behind in the canal. Nickel-titanium (NiTi) rotary files are in common usage in these days. Despite their undeniable advantages, there is a potential risk of separation within the canals. It is very rapid, unpredictable, and creates a great deal of stress for the practitioner. When an endodontic instrument separates, the best option is to remove it. Ultrasonic instruments and microscopes have improved the success rate for removing separated instruments. But it is difficult and not always possible. Therefore prevention is the key. In this case report, several management methods of separated file in the canal are presented.
Keyword
Figure
-
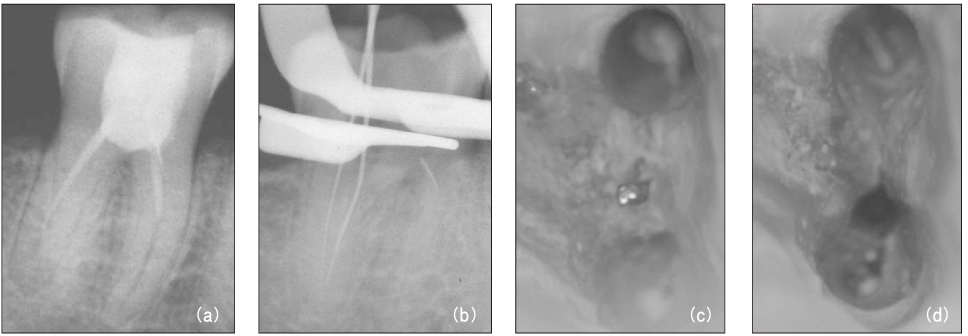
Figure 1 Diagnostic intraoral radiograph (a). Separated file in the mesial root isthmus (b, c) and remove it using ultrasonic device under microscope (d).

Figure 2 Diagnostic intraoral radiograph.

Figure 3 File separation in the root canal (a, b) and remove using ultrasonic device under microscope (c).

Figure 4 Master cone fitting and canal filling. Arrow indicates thinned dentinal wall.

Figure 5 Diagnostic intraoral radiograph.
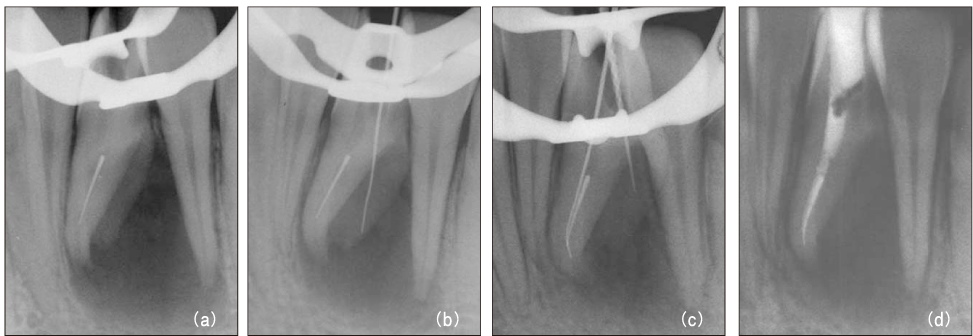
Figure 6 File separation in the canal (a) and root perforation (b). Canal obturation after bypassing with hand file (c, d).
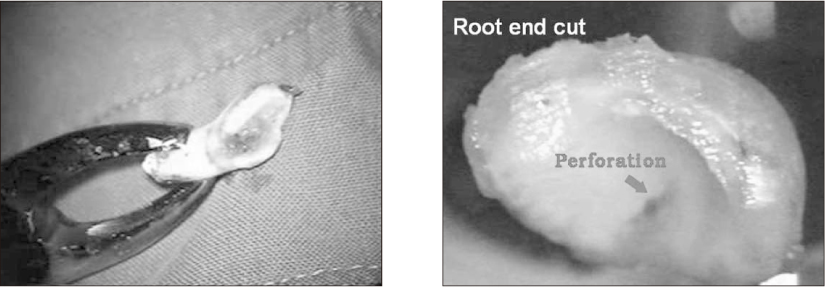
Figure 7 After tooth extraction, C-shaped root apex and root perforation were investigated.
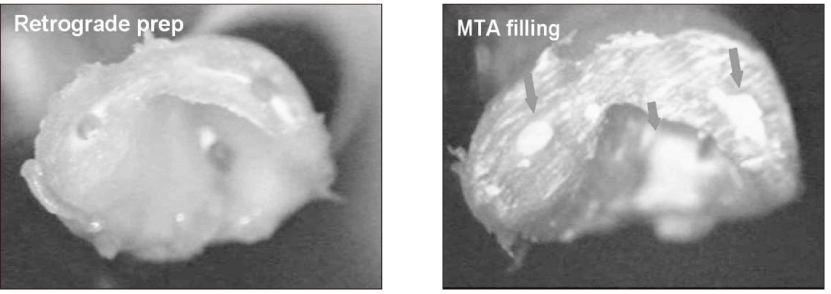
Figure 8 Retrograde preparation and MTA filling.
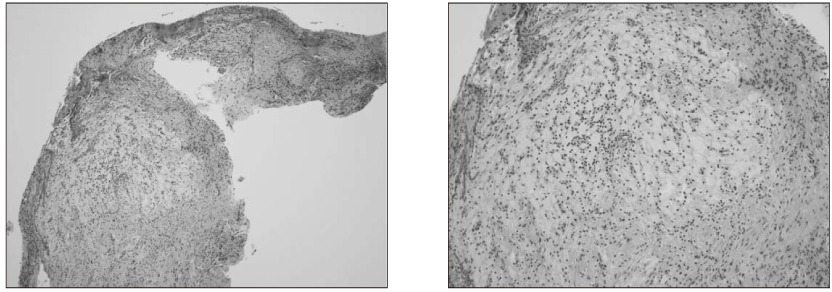
Figure 9 Histological appearance of surgically removed tissue.
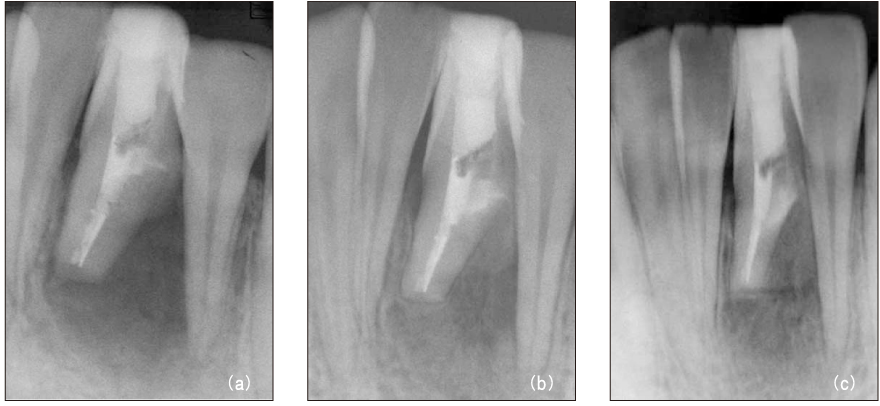
Figure 10 After intentional replantation (a), 3-month recall (b), 6-month recall (c) radiograph.

Figure 11 Diagnostic intraoral radiograph (a). By-passing with hand file (b) and canal obturation (c, d). 30-month recall (e): tooth is symptomless.
Reference
-
1. Mounce R. The heartache of separation. Dent Today. 2003. 22(4):83–85.2. Ruddle C. Cleaning and shaping the root canal system. Pathways of the Pulp. 2002. 8th ed. St. Louis: Mosby;231–292.3. Nagai O, Tani N, Kayaba Y, Kodama S, Osada T. Ultrasonic removal of broken instruments in root canals. Int Endod J. 1986. 19(6):298–304.
Article4. Hulsmann M, Schinkel I. Influence of several factors on the success or failure of removal of fractured instruments from the root canal. Endod Dent Traumatol. 1999. 15(6):252–258.
Article5. Ruddle CJ. Broken instrument removal. The endodontic challenge. Dent Today. 2002. 21(7):70–81.6. Shen Y, Peng B, Cheung GS. Factors associated with the removal of fractured NiTi instruments from root canal systems. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004. 98(5):605–610.
Article7. Ward JR, Parashos P, Messer HH. Evaluation of an ultrasonic technique to remove fractured rotary nickel-titanium endodontic instruments from root canals: an experimental study. J Endod. 2003. 29(11):756–763.
Article8. Ward JR, Parashos P, Messer HH. Evaluation of an ultrasonic technique to remove fractured rotary nickel-titanium endodontic instruments from root canals: clinical cases. J Endod. 2003. 29(11):764–767.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Selection of Nickel-Titanium Files according to the Clinical Procedure and Factors of File Fracture: A Narrative Review
- Shaping ability of nickel-titaniumrotary files
- Comparative evaluation of the effectiveness of ultrasonic tips versus the Terauchi file retrieval kit for the removal of separated endodontic instruments
- Relative efficacy of three Ni-Ti file systems used by undergraduates
- A comparison of master apical file size according to instrumentation in type II root canal
