Cause of Chest Pain in a Patient with Previous Myocardial Infarction: Look Outside the Heart for Extracardiac Mass
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea. smparkmd@korea.ac.kr
- KMID: 2172229
- DOI: http://doi.org/10.4068/cmj.2011.47.3.177
Abstract
- We report a case of thymic carcinoma that was initially detected by echocardiography in an 80-year-old male who visited the emergency room for chest pain and had a history of myocardial infarction and percutaneous coronary intervention. Transthoracic echocardiography showed a huge extracardiac mass that was located in the anterior mediastinum and was diagnosed as a thymic carcinoma by biopsy.
Keyword
MeSH Terms
Figure
-
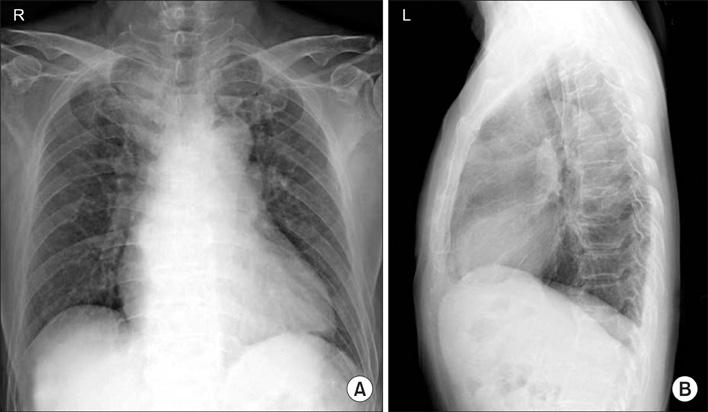
FIG. 1 Chest radiograph showed mild cardiomegaly and mediastinal widening.

FIG. 2 Hypoechogenic mass (arrow) was shown in the parasternal long axis view (A) and short-axis view at the level of the aortic valve (B).The vascularity of the mass was documented in color flow imaging in the zoom view (C). M: mass, RV: right ventricle, LV: left ventricle, LA: left atrium, AV: aortic valve, PA: pulmonary artery.
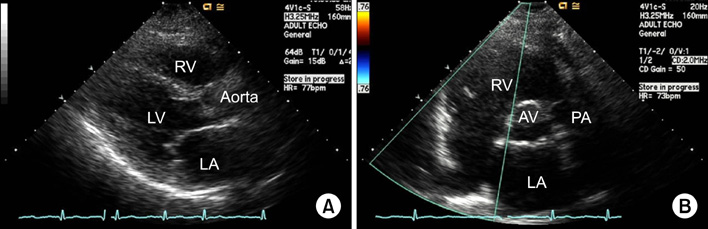
FIG. 3 Echocardiography in the parasternal long axis view (A) and short axis view at the level of the aortic valve (B) 1 year previously showed no echogenic material in the retrosternal area.

FIG. 4 Contrast-enhanced computerized tomography showed a heterogeneously enhancing mass (arrow) in the left anterior mediastinum abutting the aortic arch and pulmonary artery with sternal and costal cartilage.

FIG. 5 Using a microscope with 100× magnification, the great majority of cells had tumoral necrosis and a very small number of cells had a high nucleus to cytoplasm ratio with hyperchromatin.
Reference
-
1. Pope JH, Aufderheide TP, Ruthazer R, Woolard RH, Feldman JA, Beshansky JR, et al. Missed diagnoses of acute cardiac ischemia in the emergency department. N Engl J Med. 2000. 342:1163–1170.
Article2. Swinburn JM, Stubbs P, Soman P, Collinson P, Lahiri A, Senior R. Independent value of tissue harmonic echocardiography for risk stratification in patients with non-ST-segment elevation acute chest pain. J Am Soc Echocardiogr. 2002. 15:1031–1037.
Article3. Duwe BV, Sterman DH, Musani AI. Tumors of the mediastinum. Chest. 2005. 128:2893–2909.
Article4. Ozer N, Can I, Aytemir K, Atalar E, Erman M, Ovünç K, et al. Malignant thymoma invading the right atrium: a rare echocardiographic finding. Echocardiography. 2002. 19:61–62.
Article5. D'Cruz IA, Feghali N, Gross CM. Echocardiographic manifestations of mediastinal masses compressing or encroaching on the heart. Echocardiography. 1994. 11:523–533.6. Canedo MI, Otken L, Stefadouros MA. Echocardiographic features of cardiac compression by a thymoma simulating cardiac tamponade and obstruction of the superior vena cava. Br Heart J. 1977. 39:1038–1042.
Article7. Woldow A, Kotler M, Goldstein S, Milcu M. Thymoma with pericardial tamponade. Clin Cardiol. 1995. 18:484–485.
Article8. Sadohara J, Fujimoto K, Müller NL, Kato S, Takamori S, Ohkuma K, et al. Thymic epithelial tumors: comparison of CT and MR imaging findings of low-risk thymomas, high-risk thymomas, and thymic carcinomas. Eur J Radiol. 2006. 60:70–79.
Article9. Seto H, Kageyama M, Shimizu M, Wu YW, Kamei T, Kakishita M. Assessment of residual tumor viability in thymic carcinoma by sequential thallium-201 SPECT: comparison with CT and biopsy findings. J Nucl Med. 1994. 35:1659–1661.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Myocardial Ischemia and Myocardial Injury Caused by Coronary Vasospasm Associated with Hyperthyroidism
- Serum Myoglobin in the Early Phase of Acute Myocardial Infarction
- Left Side Otalgia Caused by Acute Myocardial Infarction
- Acute Proximal Aortic Dissection Associated with ST Segment Elevation on Electrocardiography
- Spinal Cord Infarction with Anterior Chest Pain
