Radiographic Characteristics of Adrenal Masses in Oncologic Patients
- Affiliations
-
- 1Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea. swkimmd@snu.ac.kr
- 2Department of Internal Medicine, Seoul Metropolitan Government Seoul National University Boramae Medical Center, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 2169706
- DOI: http://doi.org/10.3803/EnM.2016.31.1.147
Abstract
- BACKGROUND
We aimed to assess the usefulness of pre-contrast Hounsfield unit (HU) and mass size on computed tomography to differentiate adrenal mass found incidentally in oncologic patients.
METHODS
From 2000 to 2012, 131 oncologic patients with adrenal incidentaloma were reviewed retrospectively. Receiver operating characteristic (ROC) curves were applied to determine the optimal cut-off value of the mean HU and size for detecting adrenal metastasis.
RESULTS
The median age was 18 years, and 80 patients were male. The initial mass size was 18 mm, and 71 (54.2%) of these were on the left side. A bilateral adrenal mass was found in 11 patients (8.4%). Biochemically functional masses were observed in 9.2% of patients. Thirty-six out of 119 patients with nonfunctional masses underwent adrenalectomy, which revealed metastasis in 13. The primary cancers were lung cancer (n=4), renal cell carcinoma (n=2), lymphoma (n=2), hepatocellular carcinoma (n=2), breast cancer (n=1), and others (n=2). The area under the curve for the size and HU for clinically suspicious metastasis were 0.839 (95% confidence interval [CI], 0.761 to 0.900; P<0.001) and 0.959 (95% CI, 0.898 to 0.988; P<0.001), respectively. The cut-off value to distinguish between metastasis and benign masses were 22 mm for size and 20 for HU.
CONCLUSION
ROC curve results suggest that pre-contrast HU >20 can be used as a diagnostic reference to suggest metastasis in oncologic patients with adrenal masses.
Keyword
MeSH Terms
Figure
-
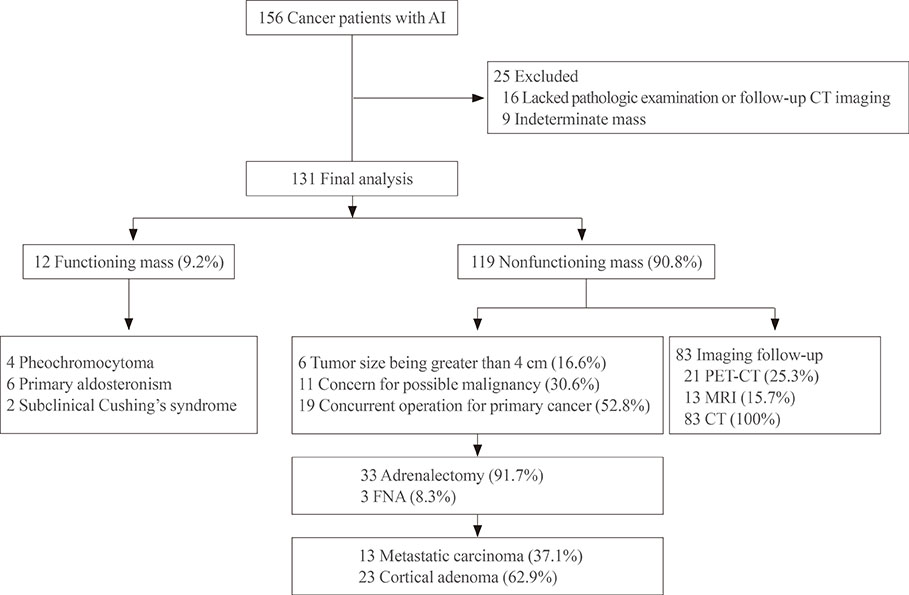
Fig. 1 Flow chart of follow-up for cancer patients with adrenal incidentaloma (AI). PET-CT, positron emission tomography-computed tomography; MRI, magnetic resonance imaging; FNA, fine needle aspiration.

Fig. 2 (A) Adrenal size and (B) Hounsfield unit (HU) for clinically suspicious benign (b) and metastasis (m).

Fig. 3 (A) Absolute percentage washout (APW) and (B) relative percentage washout (RPW) in case adrenal mass with Hounsfield unit over 10. b, clinically suspicious benign; m, clinically suspicious metastasis.

Fig. 4 Receiver operating characteristic curve for adrenal mass defined as clinically suspicious metastasis. HU, Hounsfield unit; PPV, positive predictive value; NPV, negative predictive value; AUC, area under the curve; CI, confidence interval.
Reference
-
1. Mansmann G, Lau J, Balk E, Rothberg M, Miyachi Y, Bornstein SR. The clinically inapparent adrenal mass: update in diagnosis and management. Endocr Rev. 2004; 25:309–340.2. Gittens PR Jr, Solish AF, Trabulsi EJ. Surgical management of metastatic disease to the adrenal gland. Semin Oncol. 2008; 35:172–176.3. Lumb G, Mackenzie DH. The incidence of metastases in adrenal glands and ovaries removed for carcinoma of the breast. Cancer. 1959; 12:521–526.4. Young WF Jr. Clinical practice. The incidentally discovered adrenal mass. N Engl J Med. 2007; 356:601–610.5. Kapoor A, Morris T, Rebello R. Guidelines for the management of the incidentally discovered adrenal mass. Can Urol Assoc J. 2011; 5:241–247.6. Caoili EM, Korobkin M, Francis IR, Cohan RH, Platt JF, Dunnick NR, et al. Adrenal masses: characterization with combined unenhanced and delayed enhanced CT. Radiology. 2002; 222:629–633.7. Johnson PT, Horton KM, Fishman EK. Adrenal mass imaging with multidetector CT: pathologic conditions, pearls, and pitfalls. Radiographics. 2009; 29:1333–1351.8. Anagnostis P, Karagiannis A, Tziomalos K, Kakafika AI, Athyros VG, Mikhailidis DP. Adrenal incidentaloma: a diagnostic challenge. Hormones (Athens). 2009; 8:163–184.9. Sahdev A, Reznek RH. The indeterminate adrenal mass in patients with cancer. Cancer Imaging. 2007; 7(Spec No A):S100–S109.10. Boland GW, Lee MJ, Gazelle GS, Halpern EF, McNicholas MM, Mueller PR. Characterization of adrenal masses using unenhanced CT: an analysis of the CT literature. AJR Am J Roentgenol. 1998; 171:201–204.11. Hamrahian AH, Ioachimescu AG, Remer EM, Motta-Ramirez G, Bogabathina H, Levin HS, et al. Clinical utility of noncontrast computed tomography attenuation value (hounsfield units) to differentiate adrenal adenomas/hyperplasias from nonadenomas: Cleveland Clinic experience. J Clin Endocrinol Metab. 2005; 90:871–877.12. Blake MA, Kalra MK, Sweeney AT, Lucey BC, Maher MM, Sahani DV, et al. Distinguishing benign from malignant adrenal masses: multi-detector row CT protocol with 10-minute delay. Radiology. 2006; 238:578–585.13. Grumbach MM, Biller BM, Braunstein GD, Campbell KK, Carney JA, Godley PA, et al. Management of the clinically inapparent adrenal mass ("incidentaloma"). Ann Intern Med. 2003; 138:424–429.14. Gopan T, Remer E, Hamrahian AH. Evaluating and managing adrenal incidentalomas. Cleve Clin J Med. 2006; 73:561–568.15. Lam KY, Lo CY. Metastatic tumours of the adrenal glands: a 30-year experience in a teaching hospital. Clin Endocrinol (Oxf). 2002; 56:95–101.16. Xu B, Gao J, Cui L, Wang H, Guan Z, Yao S, et al. Characterization of adrenal metastatic cancer using FDG PET/CT. Neoplasma. 2012; 59:92–99.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Usefulness of F-18 FDG PET/CT in Adrenal Incidentaloma: Differential Diagnosis of Adrenal Metastasis in Oncologic Patients
- Adrenal Incidentaloma: Imaging Approach and Differential Diagnosis
- Clinical Characteristics for 348 Patients with Adrenal Incidentaloma
- A Case of Bilateral Adrenal Masses due to Tuberculosis
- Clinical Characteristics for 132 Patients with Adrenal Incidentaloma
