Endoscopic Resection of Giant Colonic Lipoma: Case Series with Partial Resection
- Affiliations
-
- 1Digestive Disease Center, CHA Bundang Medical Center, CHA University, Seongnam, Korea. endoscopy@cha.ac.kr
Abstract
- Colonic lipoma, a very rare form of benign tumor, is typically detected incidentally in asymptomatic patients. The size of lipoma is reported variously from 2 mm to 30 cm, with higher likelihood of symptoms as the size is bigger. Cases with symptom or bigger lesion are surgically resected in principle; endoscopic resection, which has developed recently with groundbreaking advance of endoscopic excision technology, is being used more often but with rare report of success due to high chance of complications such as bowel perforation or bleeding. The authors report here, together with a literature review, our experiences of three cases of giant colonic lipomas showing complete remission after aggressive unroofing technique, at certain intervals, using snare catheter at the origin of the lipoma so that the remaining lipoma could be drained out of the exposed surface spontaneously, in order to reduce complications.
Keyword
Figure
-
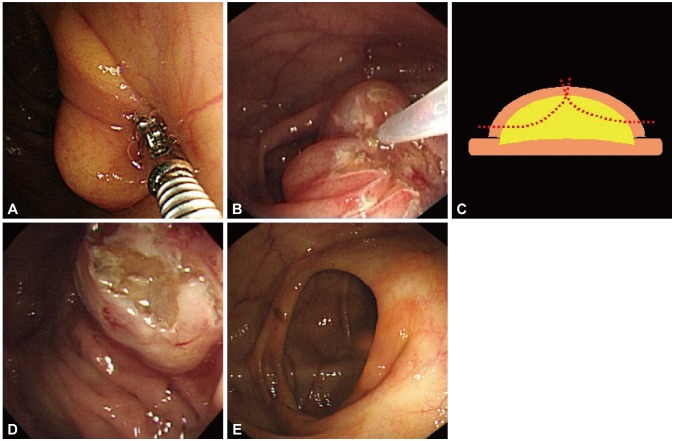
Fig. 1 Endoscopic resection of a giant colon lipoma, case 1. (A) A wide-based 3×3-cm yellowish protruding mass without mucosal change detected at the ileocecal valve during colonoscopy. (B) Partial resection with unroofing technique performed twice at the center of the lesion using snare catheter (ASM-1-S; Wilson-Cook Medical Inc.). (C) A simplified illustration of the procedure. (D) Half the mass is resected, and yellow tissue can be observed on the exposed surface of the remaining lesion, indicating typical lipoma. (E) Three-year follow-up colonoscopy. There's no remaining evidence of the lipoma, except for the surgical scar.
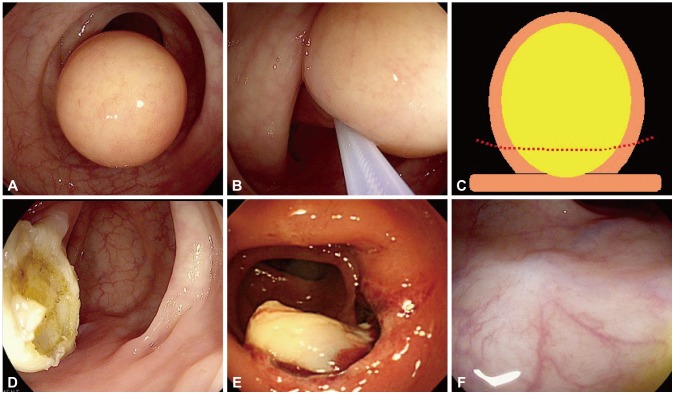
Fig. 2 Endoscopic resection of a giant colon lipoma, case 2. (A) A 3×3-cm yellowish protruding mass without mucosal change detected at the sigmoid colon during colonoscopy. (B) Partial resection performed on the center of the lesion using snare. (C) A simplified illustration of the procedure. (D) Most of the mass is resected, and yellow tissue can be observed on the exposed surface of the remaining lesion, indicating typical lipoma. (E) Colonoscopy on the next day. The remaining lipoma tissues are flowing out of the exposed lesion. (F) One-year follow-up colonoscopy. There's no remaining evidence of the lipoma, except for the surgical scar.
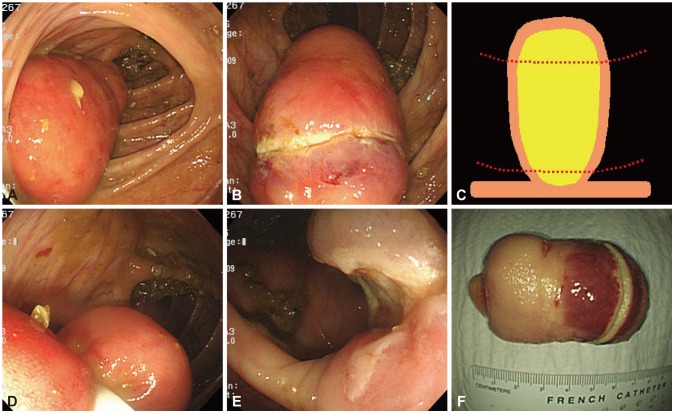
Fig. 3 Endoscopic resection of a giant colon lipoma, case 3. (A) A 4×7-cm cylindrical protruding mass without mucosal change originating from the proximal ascending colon detected during colonoscopy. (B) Partial resection at the apical end of the mass resulted in serious thermal injury on the adjacent tissues without proper conduction of the electric current. (C) A simplified illustration of the procedure. (D) Since the diameter of the mass became decreased toward the base of the cylindrical mass, partial resection was retried slightly apart from the origin. (E) Yellow tissue can be observed on the exposed surface of the remaining lesion, indicating typical lipoma. Thermal injury of the adjacent tissues is not observed. (F) The resected specimen of the mass. The apical end of the mass was too thick to apply electric current without inflicting severe thermal injury on the adjacent tissues, while the actual resected part was relatively thinner and the electric current was well-applied with rare thermal injury on the adjacent tissues.
Reference
-
1. Michowitz M, Lazebnik N, Noy S, Lazebnik R. Lipoma of the colon: a report of 22 cases. Am Surg. 1985; 51:449–454. PMID: 4026070.2. Chung YF, Ho YH, Nyam DC, Leong AF, Seow-Choen F. Management of colonic lipomas. Aust N Z J Surg. 1998; 68:133–135. PMID: 9494006.
Article3. Zhang H, Cong JC, Chen CS, Qiao L, Liu EQ. Submucous colon lipoma: a case report and review of the literature. World J Gastroenterol. 2005; 11:3167–3169. PMID: 15918213.
Article4. Tamura S, Yokoyama Y, Morita T, Tadokoro T, Higashidani Y, Onishi S. "Giant" colon lipoma: what kind of findings are necessary for the indication of endoscopic resection? Am J Gastroenterol. 2001; 96:1944–1946. PMID: 11419863.
Article5. El-Khalil T, Mourad FH, Uthman S. Sigmoid lipoma mimicking carcinoma: case report with review of diagnosis and management. Gastrointest Endosc. 2000; 51(4 Pt 1):495–496. PMID: 10744833.
Article6. Bahadursingh AM, Robbins PL, Longo WE. Giant submucosal sigmoid colon lipoma. Am J Surg. 2003; 186:81–82. PMID: 12842756.
Article7. Mimura T, Kuramoto S, Hashimoto M, et al. Unroofing for lymphangioma of the large intestine: a new approach to endoscopic treatment. Gastrointest Endosc. 1997; 46:259–263. PMID: 9378215.
Article8. Soares JB, Gonçalves R, Rolanda C. Endoscopic resection of a large colonic lipoma by unroofing technique. Endoscopy. 2011; 43(Suppl 2 UCTN):E407. PMID: 22275025.
Article9. Matsushita M, Danbara N, Kawamata S, Omiya M, Okazaki K. Endoscopic removal of large colonic lipomas: difficult submucosal dissection or easy snare unroofing? Endoscopy. 2009; 41:475–478. PMID: 19418405.
Article10. Tascilar O, Cakmak GK, Gün BD, et al. Clinical evaluation of submucosal colonic lipomas: decision making. World J Gastroenterol. 2006; 12:5075–5077. PMID: 16937511.
Article11. Pfeil SA, Weaver MG, Abdul-Karim FW, Yang P. Colonic lipomas: outcome of endoscopic removal. Gastrointest Endosc. 1990; 36:435–438. PMID: 2227312.
Article12. Nesher E, Schreiber L, Werbin N. Bauhin's ileocecal valve syndrome-a rare cause for small-bowel obstruction: report of a case. Dis Colon Rectum. 2006; 49:527–529. PMID: 16482419.
Article13. Chase MP, Yarze JC. "Giant" colon lipoma: to attempt endoscopic resection or not? Am J Gastroenterol. 2000; 95:2143–2144. PMID: 10950091.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Giant Colonic Lipoma Showing Spontaneous Resolution after Endoscopic Partial Resection
- Case of a Giant Colonic Lipoma That Was Endoscopically Removed by Strangulation with Repetitive Endoloop Ligation
- A Case of Colonic Giant Lipoma Removed by Endoscopic Resection
- A Case of a Colonic Giant Lipoma Removed by Endoscopic Resection
- A Case of Giant Colonic Lipoma Endoscopically Removed Using an Unroofing Technique in Phases
