Progress of Rehabilitation in Patients with Hypoglycemic Encephalopathy Accompanying Dysphagia and Voiding Difficulty: A Case Report
- Affiliations
-
- 1Department of Rehabilitation Medicine, Kangwon National University Hospital, Korea. sora.baek@kangwon.ac.kr
- 2Gangwon-do Rehabilitation Hospital, Korea.
- 3Department of Rehabilitation Medicine, Kangwon National University School of Medicine, Korea.
- KMID: 2165200
- DOI: http://doi.org/10.12786/bn.2015.8.2.113
Abstract
- Dysphagia and voiding difficulty after hypoglycemic encephalopathy (HE) are not well described in the literature. Additionally, the effect of rehabilitation on outcomes of HE has not been discussed enough. Here we report two cases of HE, who underwent comprehensive rehabilitative management. A 76-year-old man with HE had cognitive dysfunction, dysphagia, poor standing balance, and voiding difficulty. After rehabilitation for about 20 days, the patient's swallowing, gait, and voiding function was improved remarkably, and he could eat a tolerable diet, walk independently, and void without catheterization. However, the cognitive function changed a little. A 75-year-old woman with HE had cognitive dysfunction, impaired gait, dysphagia, and voiding difficulty. After rehabilitation for one month, the patient made progress in swallowing and gait. However, the cognitive function changed a little. After rehabilitation, the recovery of swallowing and locomotor function was rapid and satisfactory in two cases, however, the progress of cognitive function was not definite.
MeSH Terms
Figure
-
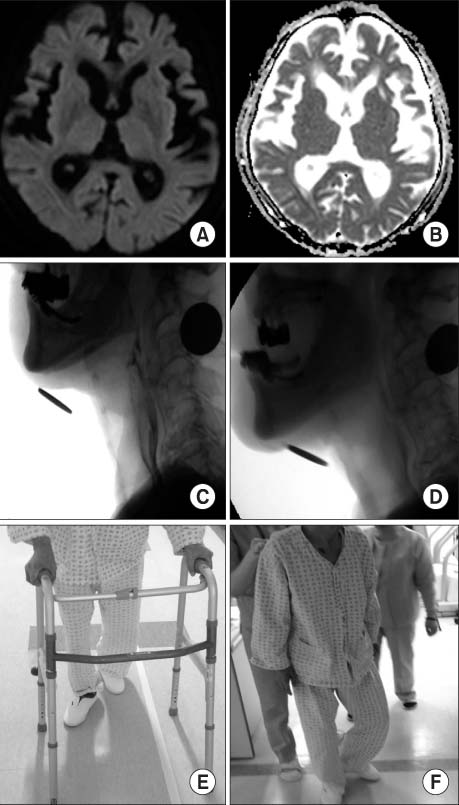
Fig. 1 Axial diffusion-weighted magnetic resonance images (A) and axial apparent diffusion coefficient maps (B) obtained 1 day after hypoglycemic attack showing small chronic ischemic lesions in the basal ganglia and deep white matter of both the hemispheres, without signs of acute lesions. An initial VFSS showing subglottic aspiration of thin fluid (C), and a follow-up VFSS showing no signs of aspiration (D). Initial standing balance is poor and gait with a walker requires minimal assistance from a physical therapist (E). After 20 days of rehabilitation, the patient is walking independently (F). VFSS: Videofluoroscopic swallowing study.
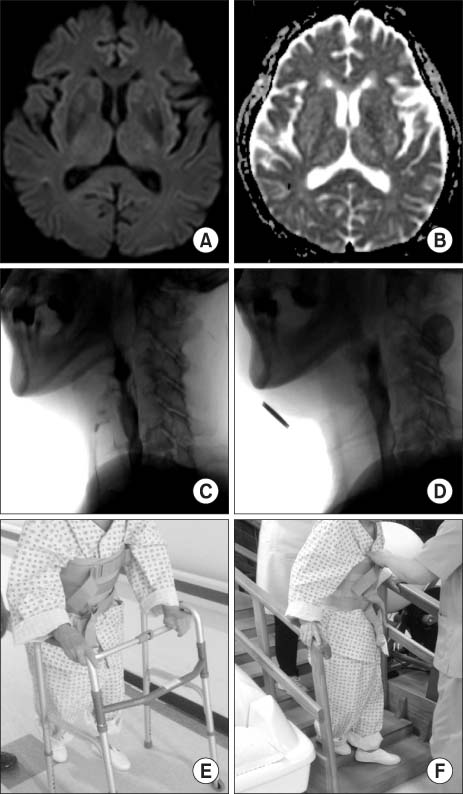
Fig. 2 Axial diffusion-weighted magnetic resonance images (A) and axial apparent diffusion coefficient maps (B) obtained 1 day after hypoglycemic attack showing multiple microbleeds in both the basal ganglia and right cerebral subcortical white matter. An initial VFSS showing subglottic aspiration of thin fluid (C), and a follow-up VFSS showing no signs of aspiration (D). Initial standing balance is poor and the patient is unable to ambulate (E). After 1 month of rehabilitation, the patient is walking with minimal assistance (F). VFSS: Videofluoroscopic swallowing study.
Reference
-
1. Malouf R, Brust JC. Hypoglycemia: causes, neurological manifestations, and outcome. Ann Neurol. 1985; 17:421–430.2. Choi JY, Seo WG, Yoo SW, Kim JH. Hypoglycemia-induced Transient Hemiparesis: Report of 2 Cases. J Korean Neurol Assoc. 2007; 25:451–453.3. Wallis WE, Donaldson I, Scott RS, Wilson J. Hypoglycemia masquerading as cerebrovascular disease (hypoglycemic hemiplegia). Ann Neurol. 1985; 18:510–512.4. Witsch J, Neugebauer H, Flechsenhar J, Juttler E. Hypoglycemic encephalopathy: a case series and literature review on outcome determination. J Neurol. 2012; 259:2172–2181.5. Ikeda T, Takahashi T, Sato A, Tanaka H, Igarashi S, Fujita N, Kuwabara T, Kanazawa M, Nishizawa M, Shimohata T. Predictors of outcome in hypoglycemic encephalopathy. Diabetes Res Clin Pract. 2013; 101:159–163.6. Kim JE, Na SJ, Lee JY, Kim YD. A Case of Hypoglycemic Encephalopathy with Lesion in the Hippocampus on Diffusion-Weighted MRI. J Korean Neurol Assoc. 2006; 24:633–635.7. Whiting DR, Guariguata L, Weil C, Shaw J. IDF diabetes atlas: global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes Res Clin Pract. 2011; 94:311–321.8. Wexler DJ, Meigs JB, Cagliero E, Nathan DM, Grant RW. Prevalence of hyper- and hypoglycemia among inpatients with diabetes: a national survey of 44 U.S. hospitals. Diabetes Care. 2007; 30:367–369.9. Sohn MK, Choi PS, Kim SK, Jee SJ, Lee TS. Hypoglycemic Encephalopathy in an Alcoholic: A case report. Brain Neurorehabil. 2008; 1:197–199.10. Kang EG, Jeon SJ, Choi SS, Song CJ, Yu IK. Diffusion MR imaging of hypoglycemic encephalopathy. AJNR Am J Neuroradiol. 2010; 31:559–564.11. Seo IK, Choi WI, Jin SC, Chang HW. Consideration of Prognostic Factors in Hypoglycemic Encephalopathy. Korean J Crit Care Med. 2012; 27:209–217.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hypoglycemic Encephalopathy in an Alcoholic: A case report
- Reversible Severe Dysphagia Presenting in Wernicke's Encephalopathy: A case report
- Rapid Regression of White Matter Changes in Hypoglycemic Encephalopathy
- Wernicke's Encephalopathy Caused by Dysphagia in Down Syndrome: A case report
- A Case of Severe Hypoglycemic Encephalopathy with Extensive Brain Lesions in Non-diabetics and Alcoholism
