Interpretation of Neonatal Chest Radiography
- Affiliations
-
- 1Department of Radiology, Kangwon National University Hospital, Chuncheon, Korea. hk2005.yoon@gmail.com
- KMID: 2164823
- DOI: http://doi.org/10.3348/jksr.2016.74.5.279
Abstract
- Plain radiographs for infants in the neonatal intensive care unit are obtained using the portable X-ray equipment in order to evaluate the neonatal lungs and also to check the position of the tubes and catheters used for monitoring critically-ill neonates. Neonatal respiratory distress is caused by a variety of medical or surgical disease conditions. Clinical information about the gestational week, respiratory symptoms, and any events during delivery is essential for interpretation of the neonatal chest radiographs. Awareness of common chest abnormality in the prematurely born or term babies is also very important for chest evaluation in the newborn. Furthermore, knowledge about complications such as air leaks and bronchopulmonary dysplasia following treatment are required to accurately inform the clinicians. The purpose of this article was to briefly review radiographic findings of chest diseases in newborns that are relatively common in daily practice.
MeSH Terms
Figure
-
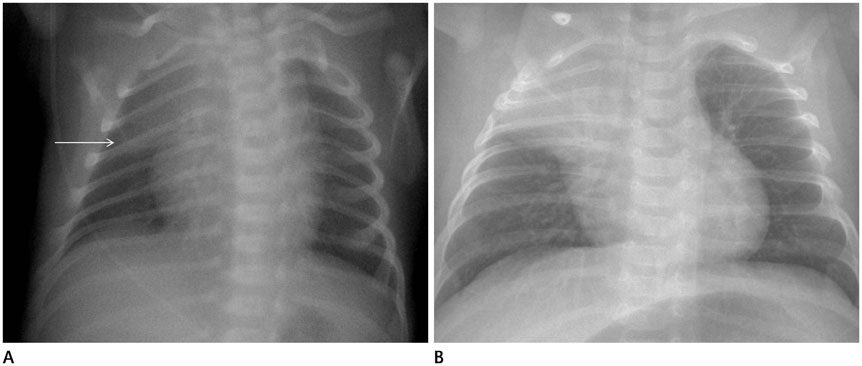
Fig. 1 Normal thymus. A. The infant is rotated and the thymic "sail" sign (arrow) is evident in the right upper mediastinum. B. This infant is also rotated and prominent thymic shadow is seen in the right upper lung field simulating right upper lobe atelectasis. Serial radiography confirmed normal thymus (not shown).

Fig. 2 Skin fold artifact. Curvilinear density is seen in the left costophrenic angle area (arrowheads), which should not be interpreted as presence of pneumothorax. Unlike pneumothorax in which the visceral pleura presents as a sharply defined line, there is a broad opacity in skin fold artifact.

Fig. 3 Umbilical arterial catheter (UAC). UAC (arrows) via the right umbilical artery goes downward first and then upward with its tip in the region of the descending thoracic aorta.
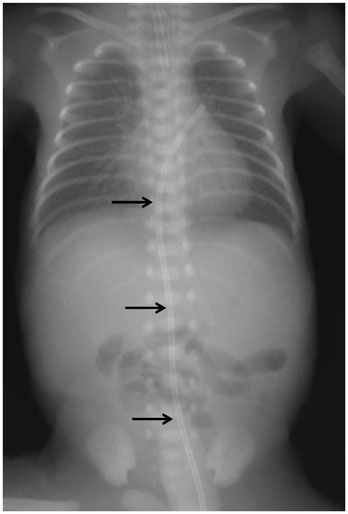
Fig. 4 Malpositioned umbilical venous catheter (UVC). Note the straight course of the UVC (arrows) from the umbilicus. The tip is malpositioned probably in the region of left upper pulmonary vein across the patent foramen ovale.
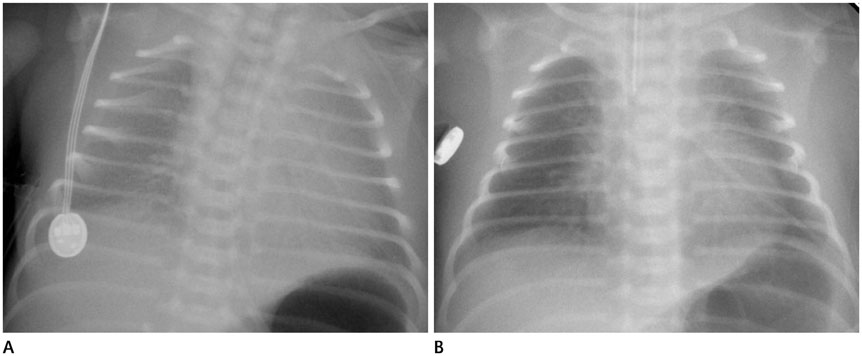
Fig. 5 Respiratory distress syndrome in a premature. A. Chest radiograph shows granular lungs with air bronchograms in the central regions. The volume of the lung is relatively small. B. After surfactant treatment, there has been clearing of lung opacities with improved aeration.
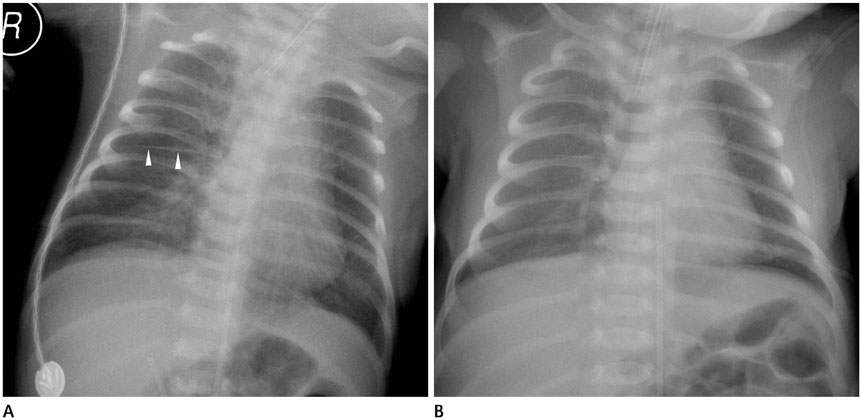
Fig. 6 Transient tachypnea of the newborn. A. Plain chest radiograph reveals overaerated lungs with radiating streaky densities from the hilum to the peripheral lungs bilaterally. Right minor fissure is accentuated (arrowheads). B. 18 hours after the initial radiography (A), there is marked interval improvement of streaky densities in the both lungs.
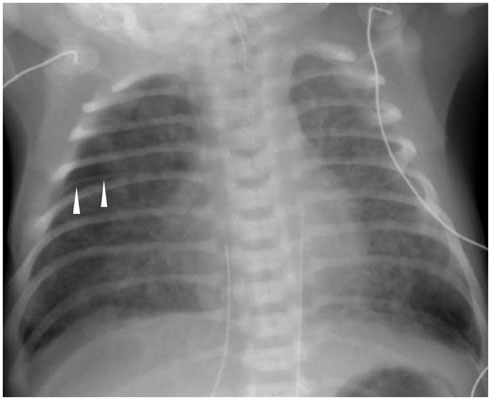
Fig. 7 Meconium aspiration syndrome. Chest radiograph demonstrates coarse irregular opacities throughout both lungs. The lungs are overinflated and the left costophrenic sulcus shows an emphysematous area. Pneumothorax is absent. The right minor fissure is accentuated, representing a small amount of pleural effusion (arrowheads).
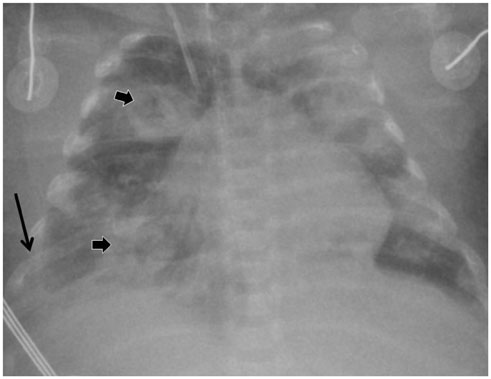
Fig. 8 Staphylococcus aureus pneumonia. Multifocal irregular opacities are observed in both lungs with cavitations (small arrows). Right pleural effusion (long arrow) is evident obliterating right costophrenic sulcus (case courtesy of Young Hun Choi, MD, Seoul National University Children's Hospital).
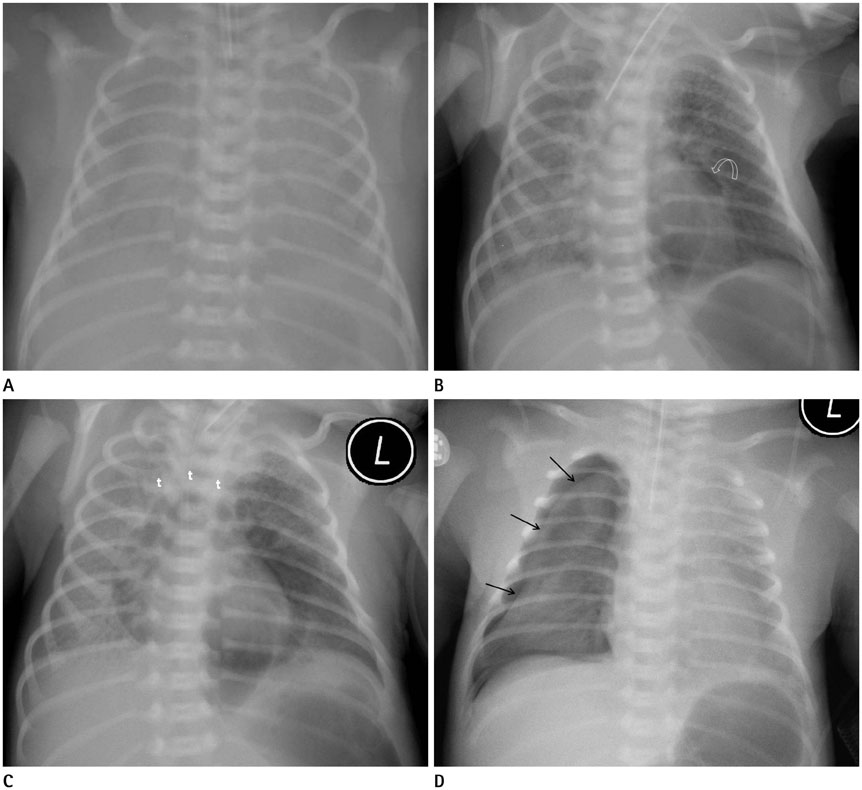
Fig. 9 Premature infant with respiratory distress syndrome (RDS) and air leaks. A. Initial chest radiograph at birth shows small and diffusely opaque lungs in keeping with severe RDS. The endotracheal tube was placed and the baby was treated with the surfactant and ventilator therapy. B-D. Follow-up chest radiographs demonstrate pulmonary interstitial emphysema (B), pneumomediastinum (C), and right sided pneumothorax (D). In (B), pulmonary interstitial emphysema appears linear and branching radiolucencies appear in the left upper lung zone together with a small amount of pneumomediastinum (curved arrow). The pneumomediastinum lines the inferior margin of the thymus in (C). In (D), the right lung is partially collapsed (arrows), which is delineated by pneumothorax. t = thymus

Fig. 10 Pneumomediastinum with inferior pulmonary ligament air. A. Chest AP radiograph shows pneumomediastinum (white arrows) with elevated thymic shadow ("angel-wing") and ovoid air density in the retrocardiac region (black arrows). B. Lateral chest radiograph confirms the location of retrocardiac air (black arrows) in the region of the inferior pulmonary ligament. Also note of pneumomediastinum (white arrow) lining the posteroinferior margin of the thymus (t). C. Follow-up chest film shows interval decrease in pneumomediastinum, as well as retrocardiac air. AP = anterior-posterior, t = thymus
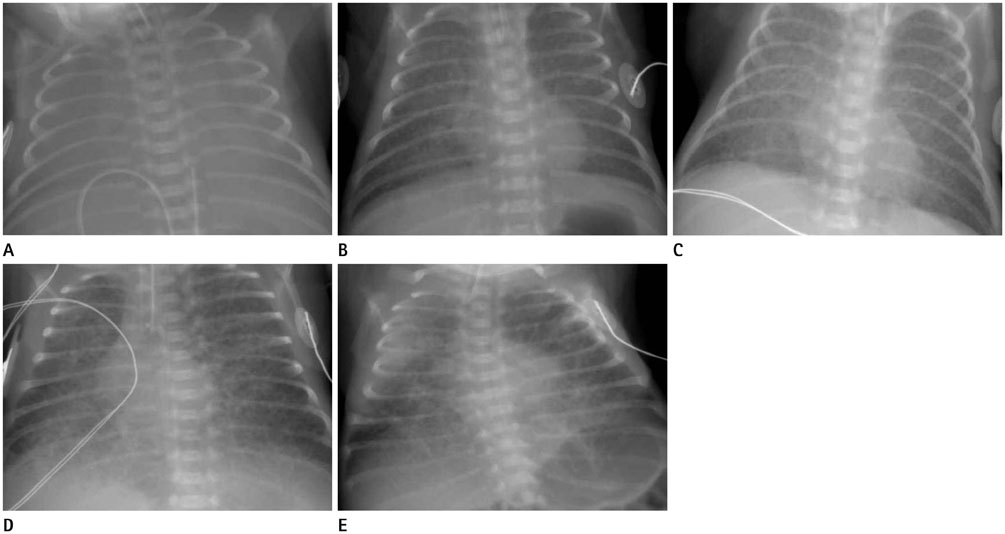
Fig. 11 Bronchopulmonary dysplasia (BPD) in a premature baby with respiratory distress syndrome (RDS). A. On chest radiograph at birth, both lungs are totally opaque, consistent with severe RDS. B-D. Serial radiographs at 1 week-interval show developing BPD changes, initially interstitial edema (B, C) to hyperinflated bubbly or cystic lungs (D). E. After two months, irregular scar-like densities with emphysema, cystic areas, and atelectasis are present. The endotracheal tube is still noted, which represents a prolonged need for oxygen.
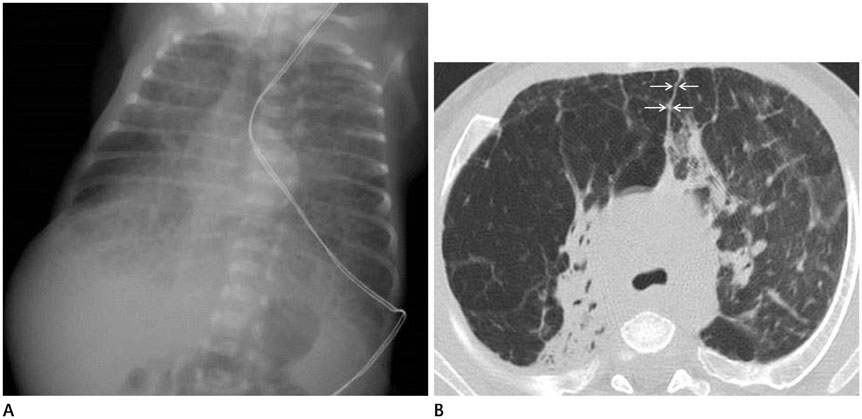
Fig. 12 A three-month-old boy with bronchopulmonary dysplasia. Plain radiograph (A) and high resolution CT (B) show emphysematous right upper lobe and multifocal atelectasis in the both lungs. The lungs are overinflated and meet together in front of the heart on CT (arrows in B).
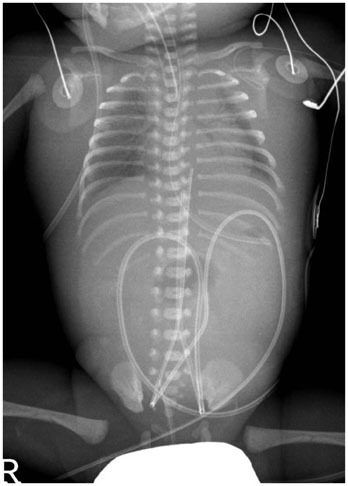
Fig. 13 Hydrops fetalis. Infantogram shows diffuse soft tissue edema and bilateral pleural effusion. Radiating strands and air bronchograms are observed in the lungs. The abdomen is almost gasless and ultrasound confirmed the presence of ascites (not shown).
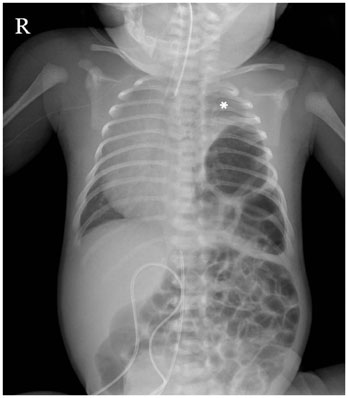
Fig. 14 Congenital diaphragmatic hernia. Air-filled bowel loops occupy the left hemithorax, compressing the heart to the opposite side. The trachea is also displaced to the right side and the small partially aerated left lung is seen in left upper hemithorax (*). Left Bochdalek hernia was confirmed at surgery.
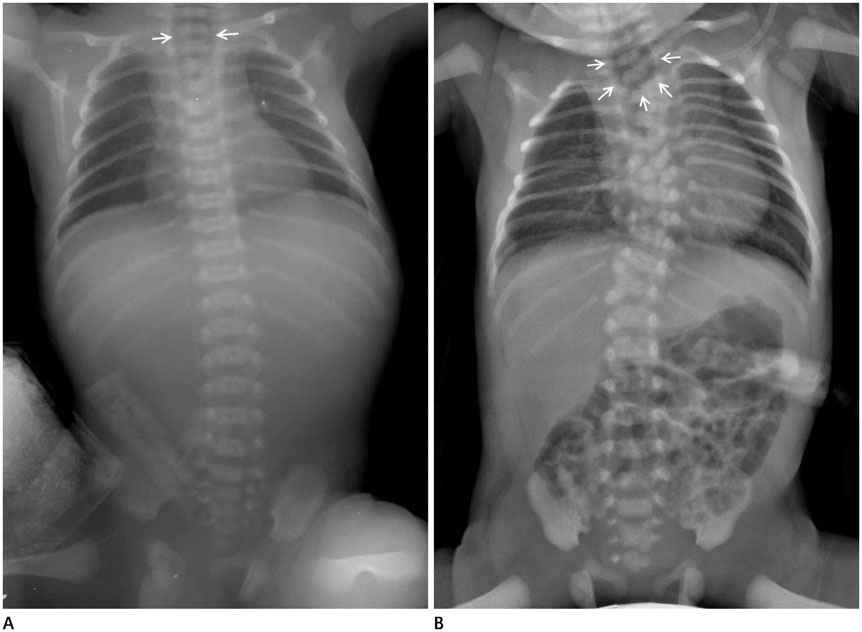
Fig. 15 Esophageal atresia. A. Esophageal atresia without distal tracheoesophageal fistula. The proximal esophagus is distended (arrows). The abdomen is completely gasless, in keeping with type A esophageal atresia without distal tracheoesophageal fistula. B. Esophageal atresia with distal tracheoesophageal fistula. As in (A), distended proximal esophagus with a loop of the gastric tube (arrows). Note the abdominal gas, representing distal tracheoesophageal fistula (type C). Segmentation anomalies are apparent in the vertebral column as well as rib anomalies, so called VATERL (Vertebral, Anorectal, TracheoEsophageal fistula, Renal, and Limb Anomalies) association.

Fig. 16 Asphyxiating thoracic dystrophy (Jeune syndrome). Plain radiography demonstrates a narrow thorax with short ribs, handle-bar clavicles, and the trident acetabulum (arrow), indicative of Jeune syndrome, a rare genetic disease.

Fig. 17 Clavicle fracture. Left clavicle mid shaft fracture is seen with callus formation (arrow).

Fig. 18 Osteogenesis imperfecta. The bony structures are diffusely osteopenic with bending of long bones involving both upper and lower extremities. Multiple fractures are also noted in both femurs. A large anterior fontanelle with intrasutural wormian bones are detected on the skull radiography (not shown).
Reference
-
1. Cleveland RH. A radiologic update on medical diseases of the newborn chest. Pediatr Radiol. 1995; 25:631–637.2. Choi YH, Kim IO. Neonatal chest imaging. In : Kim IO, editor. Radiology Illustrated: Pediatric Radiology. Berlin Heidelberg: Springer-Verlag;2014. p. 381–409.3. Kim JH, Lee YS, Kim SH, Lee SK, Lim MK, Kim HS. Does umbilical vein catheterization lead to portal venous thrombosis? Prospective US evaluation in 100 neonates. Radiology. 2001; 219:645–650.4. Agrons GA, Courtney SE, Stocker JT, Markowitz RI. From the archives of the AFIP: lung disease in premature neonates: radiologic-pathologic correlation. Radiographics. 2005; 25:1047–1073.5. Slama M, André C, Huon C, Antoun H, Adamsbaum C. Radiological analysis of hyaline membrane disease after exogenous surfactant treatment. Pediatr Radiol. 1999; 29:56–60.6. Ross MG. Meconium aspiration syndrome--more than intrapartum meconium. N Engl J Med. 2005; 353:946–948.7. Nissen MD. Congenital and neonatal pneumonia. Paediatr Respir Rev. 2007; 8:195–203.8. Bowen A 3rd, Quattromani FL. Infraazygous pneumomediastinum in the newborn. AJR Am J Roentgenol. 1980; 135:1017–1021.9. Jobe AH, Bancalari E. Bronchopulmonary dysplasia. Am J Respir Crit Care Med. 2001; 163:1723–1729.10. Howling SJ, Northway WH Jr, Hansell DM, Moss RB, Ward S, Müller NL. Pulmonary sequelae of bronchopulmonary dysplasia survivors: high-resolution CT findings. AJR Am J Roentgenol. 2000; 174:1323–1326.11. Shih YT, Su PH, Chen JY, Lee IC, Hu JM, Chang HP. Common etiologies of neonatal pleural effusion. Pediatr Neonatol. 2011; 52:251–255.12. Irish MS, Holm BA, Glick PL. Congenital diaphragmatic hernia. A historical review. Clin Perinatol. 1996; 23:625–653.
