Interrupted Inferior Vena Cava with Hemiazygos Continuation in an Adult with a Persistent Left Superior Vena Cava and Left Single Coronary Artery: A Case Report
- Affiliations
-
- 1Department of Radiology, College of Medicine, Kyung Hee University, Seoul, Korea. Kwon98@khu.ac.kr
- 2Department of Cardiology, College of Medicine, Kyung Hee University, Seoul, Korea.
- 3Department of Radiology, Kyung Hee University Hospital at Gangdong, Seoul, Korea.
- KMID: 2164817
- DOI: http://doi.org/10.3348/jksr.2016.74.6.394
Abstract
- A 50-year-old woman was referred to our institution for medical screening due to an incidental finding on abdominal ultrasonography. She underwent chest, abdomen and cardiac multi-detector computed tomography (MDCT). Her MDCT revealed absence of the hepatic segment of the inferior vena cava (IVC), with hemiazygos continuation and a left single coronary artery. The dilated hemiazygos vein drained directly into the persistent left superior vena cava (SVC). Herein, we reported a very rare case combining an incidentally found interrupted IVC with hemiazygos vein continuation, persistent left SVC and a left single coronary artery diagnosed by MDCT.
MeSH Terms
Figure
-

Fig. 1 Axial (A-C) and three-dimensional computed tomography (D) images showing an absent hepatic segment of the inferior vena cava (IVC) with hemiazygos continuation. The dilated hemiazygos vein (HAV) drains into the persistent left superior vena cava (LSVC). The LSVC drains into the right atrium through the dilated coronary sinus (CS). Hepatic veins (HVs) form a confluence and drain directly into the right atrium via supra-hepatic IVC (SH-IVC). RSVC = right superior vena cava
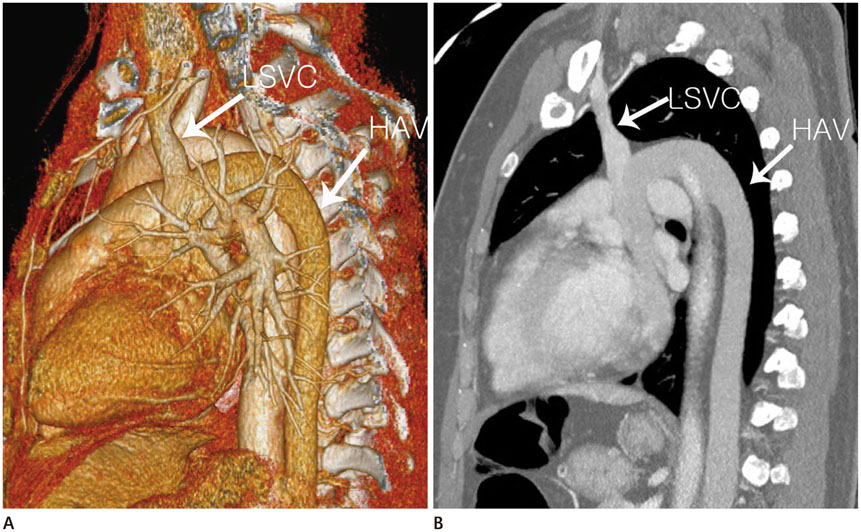
Fig. 2 Three-dimensional volume-rendering (A) and oblique sagittal maximum intensity (B) images showing the dilated hemiazygos vein (HAV) draining into the LSVC. LSVC = left superior vena cava
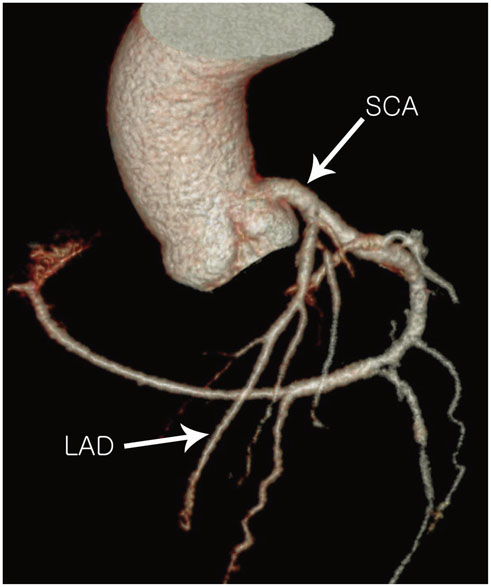
Fig. 3 Three-dimensional volume-rendering image showing the single coronary artery (SCA) arising from the left coronary sinus of Valsalva, and absence of the right coronary artery. LAD = left anterior descending artery
Reference
-
1. Yilmaz E, Gulcu A, Sal S, Obuz F. Interruption of the inferior vena cava with azygos/hemiazygos continuation accompanied by distinct renal vein anomalies: MRA and CT assessment. Abdom Imaging. 2003; 28:392–394.2. Vijayvergiya R, Bhat MN, Kumar RM, Vivekanand SG, Grover A. Azygos continuation of interrupted inferior vena cava in association with sick sinus syndrome. Heart. 2005; 91:e26.3. Yildiz AE, Cayci FS, Genc S, Cakar N, Fitoz S. Right nutcracker syndrome associated with left-sided inferior vena cava, hemiazygos continuation and persistant left superior vena cava: a rare combination. Clin Imaging. 2014; 38:340–345.4. Desmet W, Vanhaecke J, Vrolix M, Van de Werf F, Piessens J, Willems J, et al. Isolated single coronary artery: a review of 50,000 consecutive coronary angiographies. Eur Heart J. 1992; 13:1637–1640.5. Tubau A, Grau J, Filgueira A, Juan M, Estremera A, Ferrer MI, et al. Prenatal and postnatal imaging in isolated interruption of the inferior vena cava with azygos continuation. Prenat Diagn. 2006; 26:872–874.6. Minniti S, Visentini S, Procacci C. Congenital anomalies of the venae cavae: embryological origin, imaging features and report of three new variants. Eur Radiol. 2002; 12:2040–2055.7. Lipton MJ, Barry WH, Obrez I, Silverman JF, Wexler L. Isolated single coronary artery: diagnosis, angiographic classification, and clinical significance. Radiology. 1979; 130:39–47.8. Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn. 1990; 21:28–40.9. Imamura M, Abraham B, Garcia X, Knecht KR, Frazier E, Shinkawa T. New transplant technique with hemiazygos continuation and interrupted inferior vena cava. Ann Thorac Surg. 2013; 96:1882–1884.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of hemiazygos continuation of a left inferior vena cava
- A Case of Persistent Left Superior Vena Cava with Interruption of Inferior Vena Cava
- Hemiazygos Continuation of Left Inferior Vena Cava Draining into the Right Atrium via Persistent Left Superior Vena Cava: A Variant of Polysplenia Syndrome Mimicking Aortic Dissection
- Congenital Absence of the Azygos Vein with Persistent Left Superior Vena Cava: A Case Report
- Persistent Left Superior Vena Cava with Absent Right Superior Vena Cava and Large Atrial Septal Defect in Visceroatrial Situs solitus
