A study on the difference analysis between an ideal and a clinical shape in case of manufacturing a metal-ceramic pontic substructure
- Affiliations
-
- 1Department of Dental Technology and Science, Shin-Han University, Uijeongbu, Republic of Korea. wrdeul@hanmail.net
- 2Department and Research Institute of Dental Bioengineering, Yonsei University, Seoul, Republic of Korea.
- KMID: 2162374
- DOI: http://doi.org/10.14368/jdras.2016.32.1.8
Abstract
- PURPOSE
The purpose of this research is to determine whether pontic metal substructures, which are currently used in clinical surgeries, are designed appropriately and identify the problems that can occur due to their shape, size, and position. Then it aimed to emphasize the importance of making and designing pontic metal substructures based on basic principles.
MATERIALS AND METHODS
This research measured pontic basal surface (P1) used sample metal substructures in this study, gingiva margin (P2), and the porcelain thickness of maximum infrabulge of labial surface around 1/3 of cervix dentis (P3). One-way ANOVA analysis was carried out to test the differences among groups, Tukey Honestly Significant Difference Test was conducted for statistical analysis among groups.
RESULTS
For porcelain thickness and SD value, the P1 part was 1.2 - 1.8 (±0.17) mm for experimental group 1, 1.2 - 1.7 (±0.17) mm for experimental group 2, and 0.4 - 2.8 (±0.92) mm for experimental group 3. Next, the P2 part was 1.4 - 1.6 (±0.07) mm for experimental group 1, 1.3 - 1.8 (±0.07) mm for experimental group 2, and 0.5 - 2.7 (±0.67) mm for experimental group 3. The P3 part was 1.4 - 1.7 (±0.10) mm for experimental group 1, 1.5 - 2 (±0.10) mm for experimental group 2, and 0.9 - 3.1 mm (±0.90) for experimental group 3. There was no significance when One-way ANOVA analysis/Tukey Honestly Significant Difference Test was conducted for statistical analysis among groups (P > 0.05).
CONCLUSION
The suggested metal substructures can be used clinically as they meet the requirements that pontic must have.
Figure
-
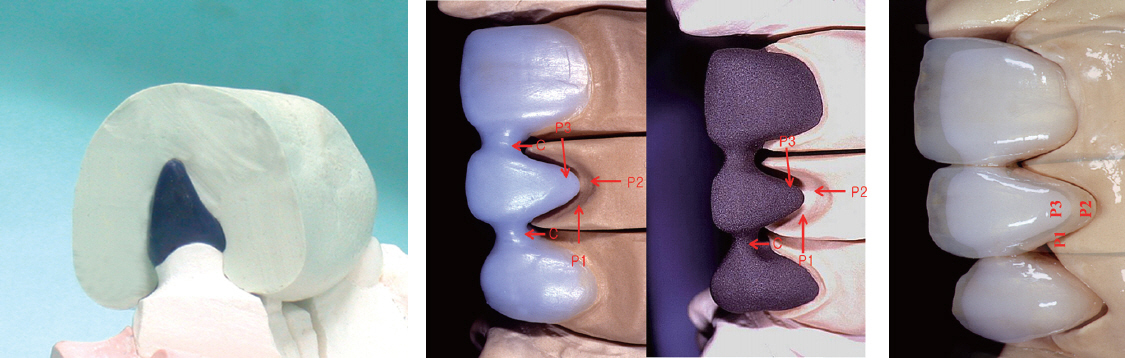
Fig. 1 Making of specimens. P1, pontic base; P2, cervical margin; P3, emergence profile; C, inter proximal.
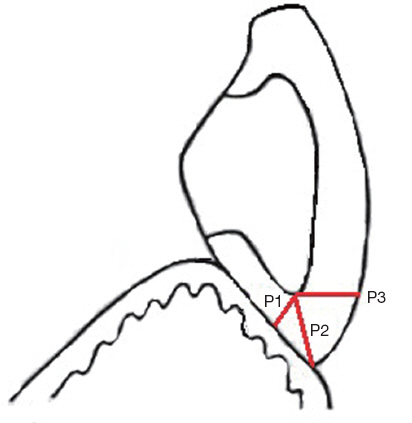
Fig. 2 Measurement position. P1, pontic base; P2, cervical margin; P3, emergence profile.
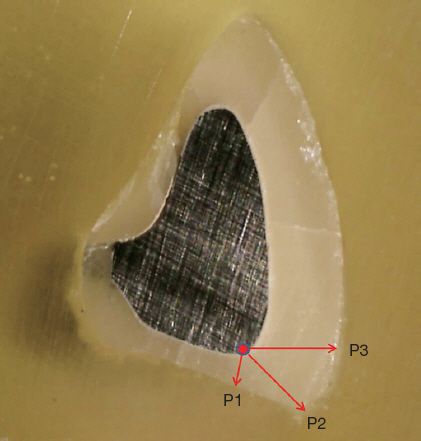
Fig. 3 Measurement of metal-ceramic thickness (magnification ×160). P1, pontic base; P2, cervical margin; P3, emergence profile.
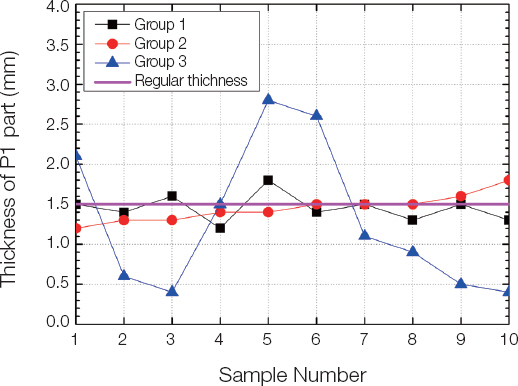
Fig. 4 The porcelain thickness of P1 part of experimental groups 1, 2, and 3.
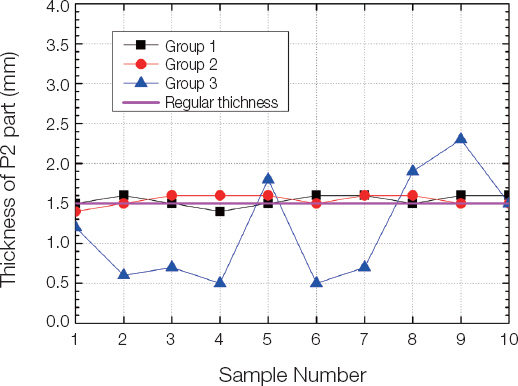
Fig. 5 The porcelain thickness of P2 part of experimental groups 1, 2, and 3.
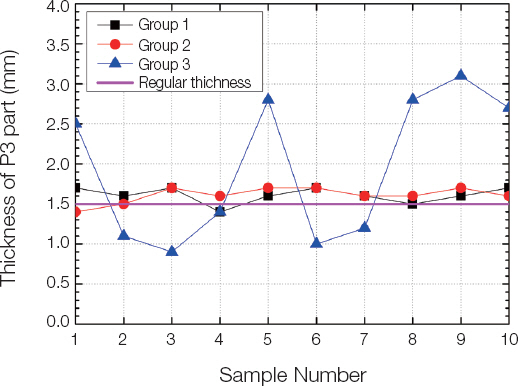
Fig. 6 The porcelain thickness of P3 part of experimental groups 1, 2, and 3.
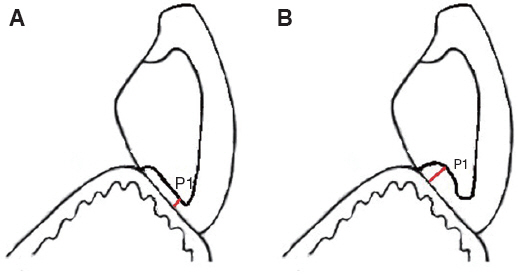
Fig. 7 Problems that can occur in P1 part when designing metal substructures. (A) It is occurred metal exposure and poor cleaning when metal substructures are close to the gingiva, (B) It’s occurred pressured inter proximal when the basal surface of metal substructures are removed straightforwardly. P1, pontic base.
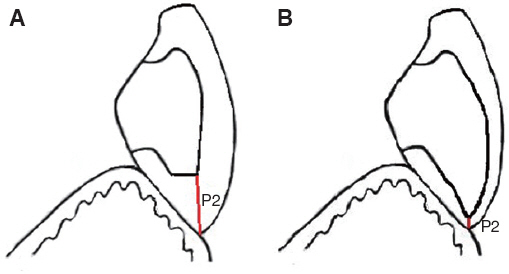
Fig. 8 Problems that can occur in P2 part when designing metal substructures. (A) It’s occurred fracture and color difference when metal substructures are short, (B) It’s occurred opaque colors shine when metal substructures are long. P2, cervical margin.
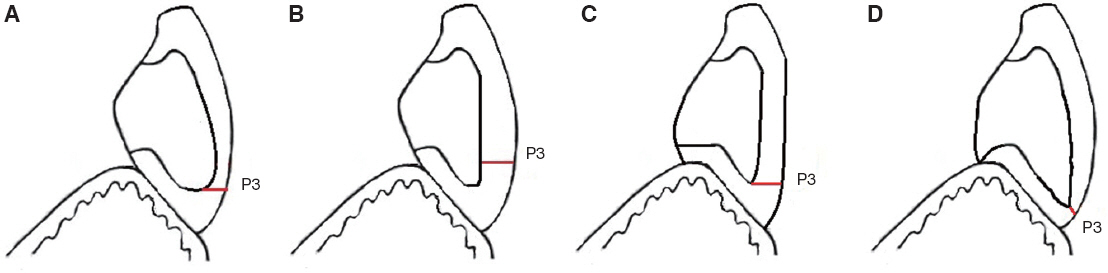
Fig. 9 Problems that can occur in P3 part when designing metal substructures. (A) It’s occurred impact hue when the metal substructures protrude, (B) It’s occurred labio-version when metal substructure is straight, (C) It’s made saddle type when metal substructures are made to face the lingual side too much, (D) It’s occurred crack and color difference when metal substructures are made long straightforwardly. P3, emergence profile.
Reference
-
References
1. Kim JB, Kim KS, Kim YH, Jeong SH, Jin BH, Chio EM, Hwang YS. Public oral health. 2004. 3rd ed. Seoul: KMS;p. 223–76. PMCID: PMC2822303.2. Silver M, Haward MC, Klein G. Porcelain bonded to a cast metal understructure. J Prosthet Dent. 1961; 11:132–45. DOI: 10.1016/0022-3913(61)90120-2.3. Hobo S, Shillingburg HT Jr. Porcelain fused to metal: tooth preparation and coping design. J Prosthet Dent. 1973; 30:28–36. DOI: 10.1016/0022-3913(73)90075-9.4. Miler LL. Framework design in ceramo-metal restorations. Dent Clin North Am. 1977; 21:699–716.5. Shelby DS. Practical considerations and design of porcelain fused to metal. J Prosthet Dent. 1962; 12:542–48. DOI: 10.1016/0022-3913(62)90137-3.6. Straussberg G, Katz G, Kuwata M. Design of gold supporting structures for fused porcelain restorations. J Prosthet Dent. 1966; 16:928–36. DOI: 10.1016/0022-3913(66)90015-1.7. Faucher RR, Nicholls JI. Distortion related to margin design in porcelain fused to metal restorations. J Prosthet Dent. 1980; 43:149–55. DOI: 10.1016/0022-3913(80)90178-X.8. Tylman SD. Theory and practice of crown and bridge prosthodontics. 1965. 5th ed. St. Louis: C V Mosby;p. 23–24.9. Kim WT. Applying the new technology for making pontic ridge lap in posterior bridge restoration. J Dent Rehabil Appl Sci. 2013; 29:308–16. DOI: 10.14368/jdras.2013.29.3.308.10. Yang JH. Technical consideration for ceramo-metal restorations. J Korean Dent Assoc. 1981; 9:339–42.11. Brecker SC. Porcelain baked to gold. A new medium in Prosthodontics. J Prosthet Dent. 1956; 6:801–10. DOI: 10.1016/0022-3913(56)90077-4.12. McLean JW. The science and art of dental ceramics. 1979. Chicago: Quintescence;p. 149–56.13. Warpeha WS Jr, Goodkind RJ. Design and technique variables affecting fracture resistance of metalceramic restorations. J Prosthet Dent. 1976; 35:291–8. DOI: 10.1016/0022-3913(76)90253-5.14. Sillness J. Fixed prosthodontics and periodontal health. Dent Clin North Am. 1980; 24:317–29.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Spectrophotometic analysis of the influence of substrate on the color of dental ceramics
- Validity experiment of dipping method in the manufacture of metalceramic substructure
- Fabricating a Ceramic-Pressed-to-Metal Restoration with Computer-Aided Design, Computer-Aided Manufacturing and Selective Laser Sintering: A Case Report
- Effect of the shades of background substructures on the overall color of zirconia-based all-ceramic crowns
- A study on frictional resistance force of orthodontic resin bracket
