Imaging and Pathologic Characterization of the Skin Thickening or Enhancement under the Breast MRI
- Affiliations
-
- 1Department of Radiology, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. lionmain@catholic.ac.kr
- KMID: 2161366
- DOI: http://doi.org/10.13104/imri.2016.20.1.9
Abstract
- The purpose of this paper is to show the radiologic features of various lesions appearing as skin thickening or enhancement under the breast MRI. And histopathologic results of the skin lesions were correlated. Radiologist must be familiar with normal appearance of the breast skin under the MRI and a wide variety of conditions may affect the skin of the breast.
Keyword
Figure
-
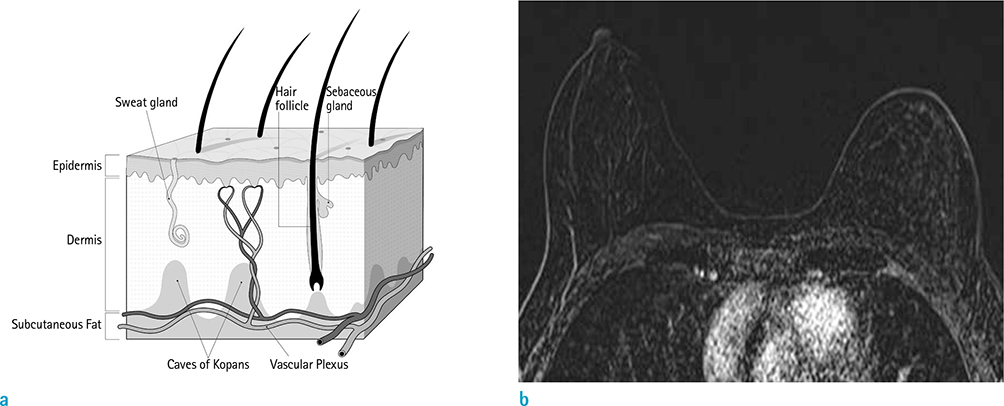
Fig. 1 Normal breast. (a) Diagram of skin. (b) On axial subtraction breast MRI obtained after administration of gadolinium contrast material shows normal skin with mild and smooth enhancement.
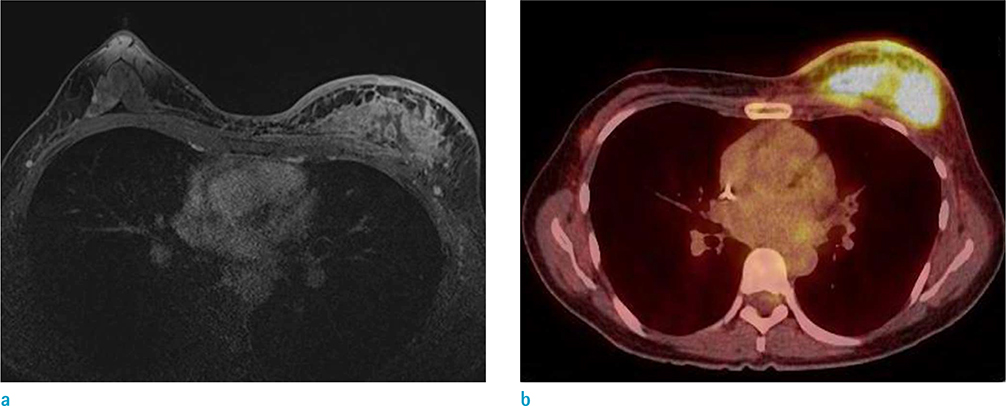
Fig. 2 A 46-year-old woman with inflammatory caner involving left breast underwent breast MRI and PET-CT. (a) On axial breast MRI, diffuse heterogeneous nonmass enhancement and diffuse skin thickening with enhancement at left breast is seen. There is irregular enhancement of the pectoralis muscle suggesting invasion. The kinetic curve of skin shows persistent enhancement pattern. (b) On PET-CT, huge mass with intense FDG uptake is seen in left breast (SUVmax 10.1) and diffuse and mild FDG uptake is also seen on breast skin (SUVmax 4.3).
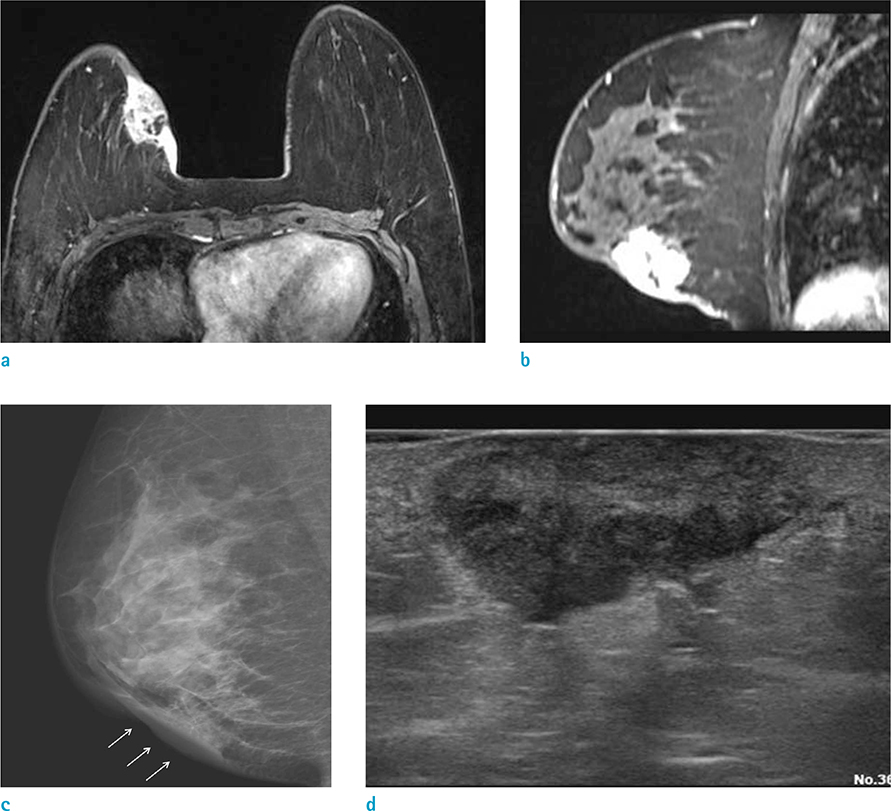
Fig. 3 A 39-year-old woman, underwent excision of florid ductal hyperplasia, 9 years before. There was thickening at the skin layer of excision site, and the punch biopsy revealed invasive ductal cancer. (a, b) On axial and sagittal breast MRI, irregular enhancing mass with direct skin invasion is seen. Focal skin thickening with enhancement is clearly seen. (c, d) On right mediolateral view of mammography and US, mass with direct skin invasion (arrows) is also seen.
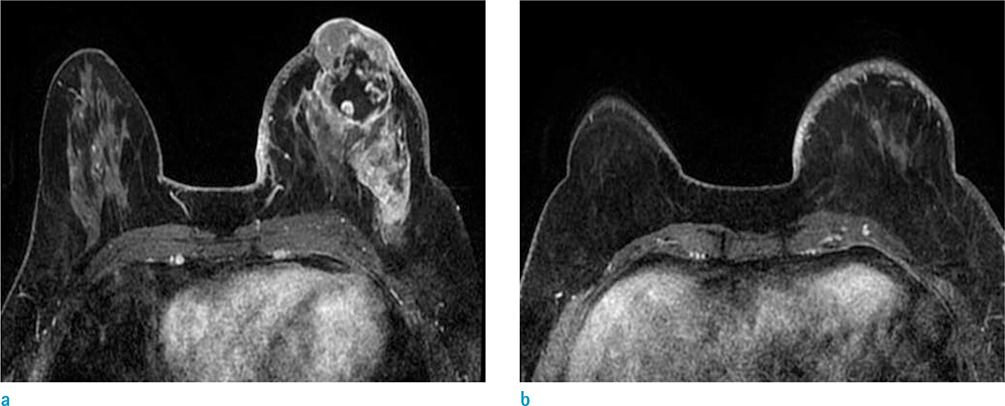
Fig. 4 A 50-year-old woman with invasive ductal cancer involving left breast underwent breast MRI and PET-CT. (a, b) On axial breast MRI, irregular and huge infiltrative enhancing mass with direct skin invasion and enhancement is seen. Nipple and areolar complex is also involved. Skin thickening and enhancement is diffuse, over third of breast skin is involved. (c) On PET-CT image, the mass with FDG uptake is seen (SUVmax 18.4) and diffuse and mild FDG uptake is seen on overlying skin.
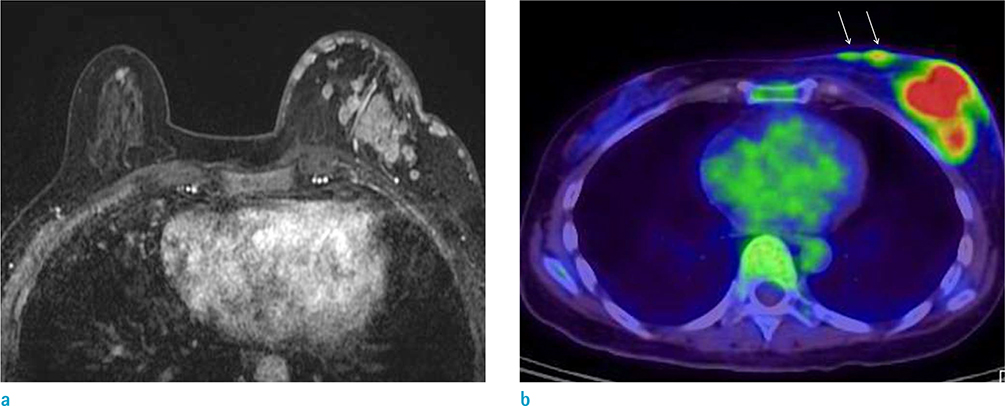
Fig. 5 A 62-year-old woman with mixed invasive ductal and mucinous cancer involving left breast underwent breast MRI and PET-CT. (a) On axial breast MRI, multiple conglomerated masses at upper outer quadrant of left breast and multiple skin nodules are clearly seen. Kinetic curve of skin nodules shows fast rise and delayed plateau pattern. (b) On PET-CT image, the mass with FDG uptake (SUVmax 8.8) is seen at left breast. And a few skin nodules with mild FDG uptake (arrows) is also seen.

Fig. 6 A 41-year-old woman, who was detected breast cancer because of palpable mass with skin ulceration. (a, b) On axial breast MRI, irregular enhancing mass with direct skin invasion and enhancement is seen. And defect of overlying skin is clearly seen, which is considered T4b stage.

Fig. 7 A 70-year-old woman with invasive lobular cancer involving right breast underwent breast MRI. (a, b) On axial breast MRI, segmental clumped nonmass enhancement is seen at upper portion of right breast. Diffuse skin thickening and enhancement is seen in right breast. (c) On clinical photography, multiple ipsilateral satellite skin nodules are seen, which is correlated with MRI detected skin thickening. The patient underwent punch biopsy of skin nodules, the pathologic result was poorly differentiated cancer originated breast cancer.

Fig. 8 A 46-year-old woman who underwent wide excision of right breast 13 months before due to invasive ductal cancer. She complained newly developed skin nodules and underwent punch biopsy for them. Pathology revealed metastatic cancer. (a, b) On axial breast MRI, multifocal irregular enhancing masses (open arrows) surrounding postoperative hematoma in right breast, suggesting recurrent tumor. The masses at anterior portion of the hematoma directly invades of skin. And multiple skin nodules with diffuse skin thickening (arrows) are clearly seen. (c) On PET-CT, the skin thickening and skin nodules show FDG uptake (SUVmax 15.7). (d) On clinical photograph of right breast, focal skin thickening and erythema around the nipple is correlated with direct skin invasion of recurrent tumor. And several skin nodules at mid inner portion of breast are correlated with nodular skin thickening on breast MRI.
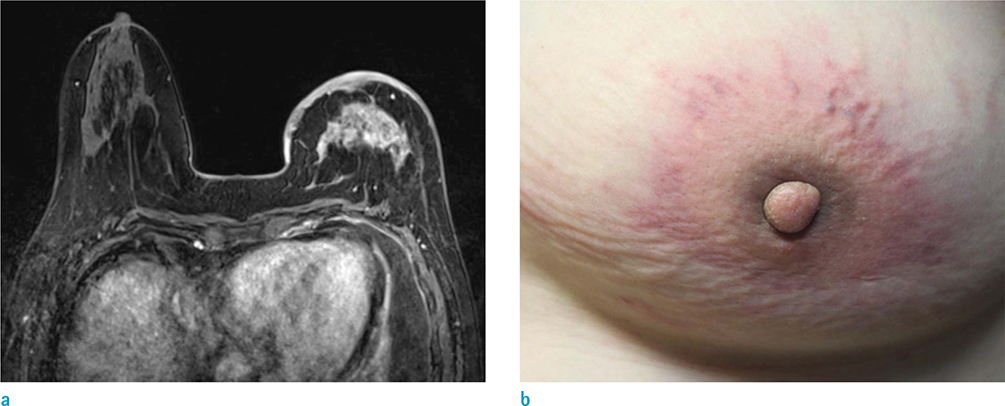
Fig. 9 A 56-year-old woman, who underwent chemotherapy due to advanced gastric cancer, complained of swelling and erythema of left breast. She underwent punch biopsy of the skin lesion and pathologic result was metastatic cancer. (a) On axial breast MRI, irregular heterogeneous enhancing mass with skin thickening and enhancement on left breast is evident. These findings mimic inflammatory breast cancer. (b) On clinical photography of left breast, breast swelling and erythema around the nipple is correlated with skin invasion of metastatic tumor.
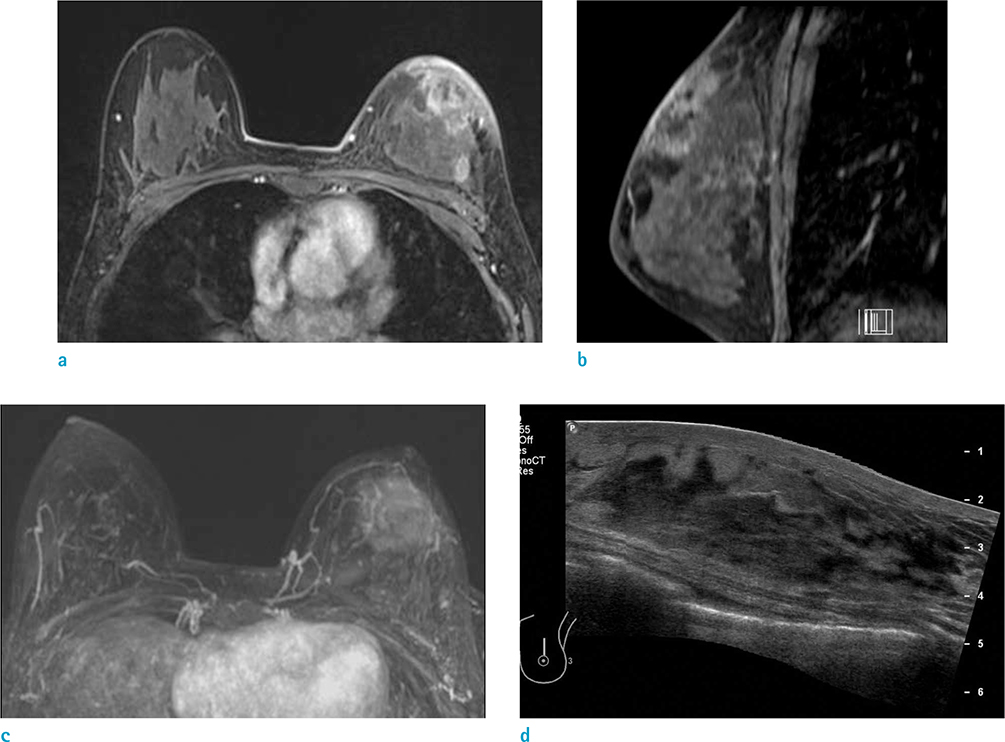
Fig. 10 A 14-year-old girl visited the out-patient clinic for evaluation of pain and palpable mass on her left breast. She underwent core needle biopsy and pathologic result was primary cutaneous extranodal NK/T cell lymphoma. (a, b) On axial and sagittal breast MRI, irregular heterogeneous enhancing mass with skin thickening and enhancement on left breast is evident. (c) Maximal intensity projection image shows mass with skin invasion clearly. (d) On US image, irregular hyperechoic mass with indistinct margin at left breast was evident.

Fig. 11 A 53-year-old woman visited outpatient clinic for evaluation of palpable masses on both breasts. She underwent core needle biopsy and pathologic result was primary breast lymphoma, diffuse large B cell lymphoma. (a) On axial breast MRI, huge irregular enhancing masses at both breasts with diffuse enhancing skin thickening are evident. (b) On US image of left breast, diffuse skin thickening and huge irregular heterogeneous echoic mass are also seen.

Fig. 12 A 40-year-old woman visited outpatient clinic because of pain, erythema and edema on her left breast. She underwent core needle biopsy for left breast, pathologic result was acute and chronic mastitis with microabscess formation and vague granulomas with multinucleated giant cells. (a) On axial breast MRI, diffuse skin thickening with enhancement is seen on her left breast. Diffuse heterogeneous enhancement with trabecular thickening on left breast consistent with acute mastitis. (b) On US image, insinuating irregular hypoechoic lesion with increased echogenicity of subcutaneous fat layer and overlying diffuse skin thickening are seen.
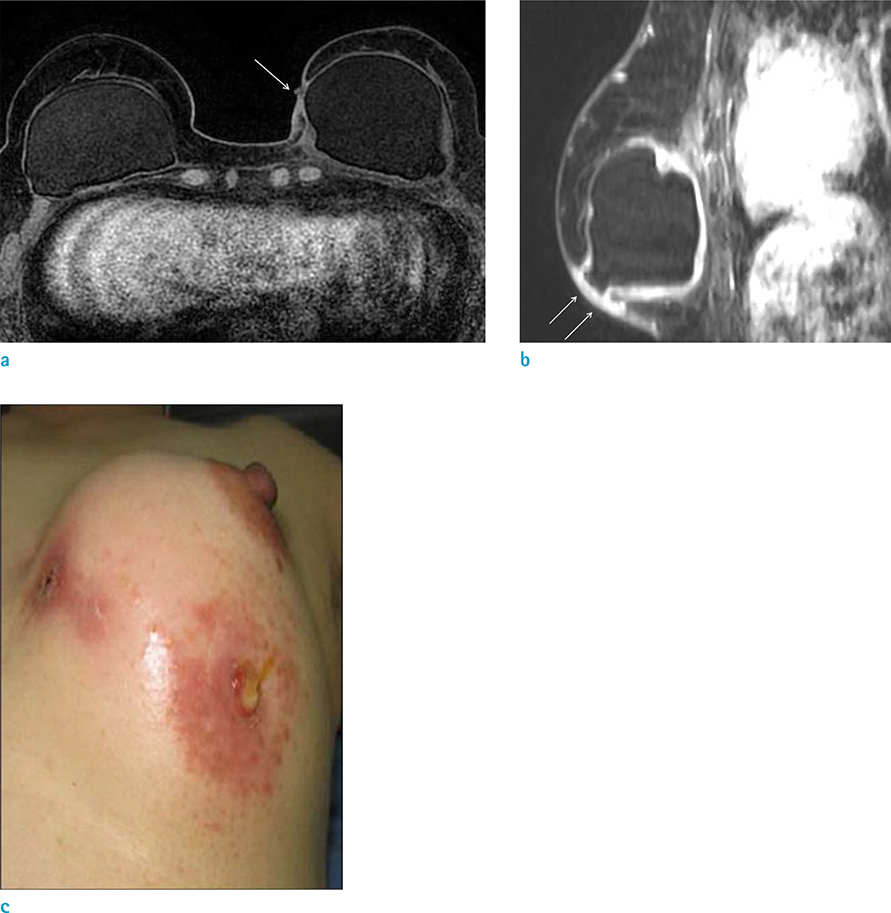
Fig. 13 A 54-year-old woman, who underwent mammoplasty with saline bag, visited outpatient clinic because of pain, erythema and pus drainage on her left breast. (a, b) On axial and sagittal breast MRI, focal skin thickening with fistula tract (arrows) is seen on her left breast. (c) On clinical photography, erythema with two, fistula tracts are seen on her left breast, which is consistent with MRI finding.
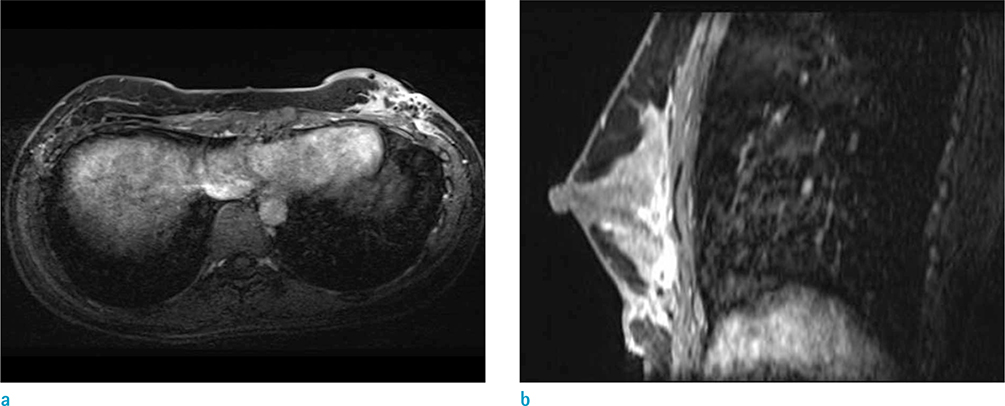
Fig. 14 A 33-year-old woman visited outpatient clinic because of pain and swelling after autologous fat injection on her breasts. She underwent debridement and curettage of left breast. (a, b) On axial and sagittal breast MRI, ill-defined soft tissue infiltration with enhancement along the retromammary space at left breast is seen, which is suggestive of inflammation with abscess formation. Diffuse skin thickening with enhancement and dark signal void of air is clearly seen.
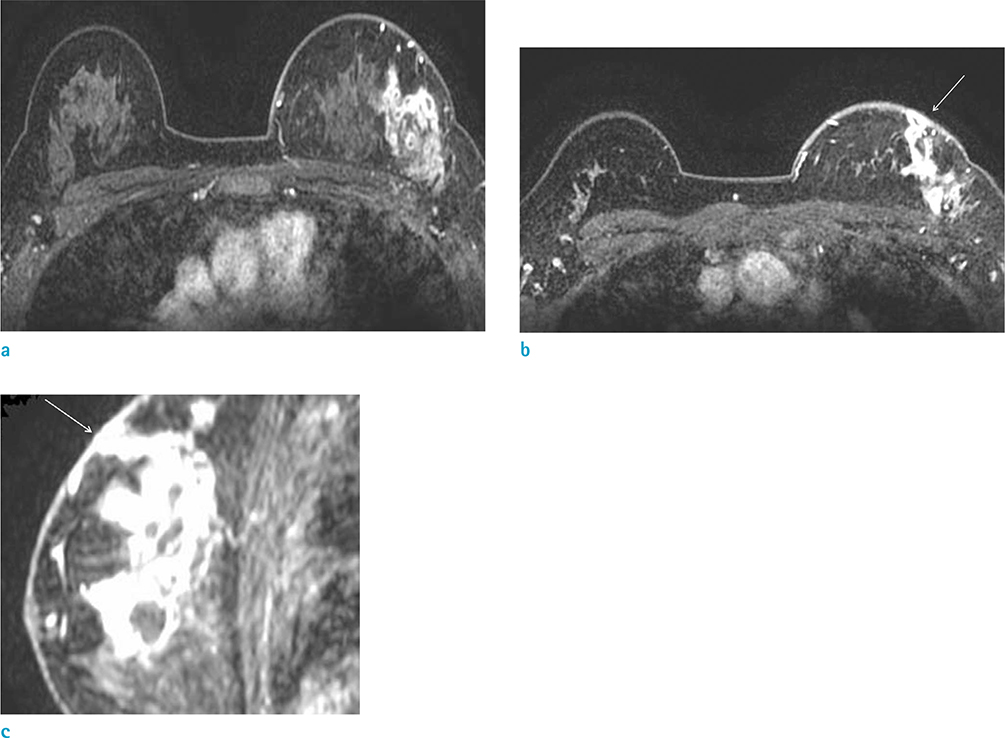
Fig. 15 A 41-year-old woman, who suffered from recurrent erythema and painful swelling on her breast, visited outpatient clinic. She underwent breast core needle biopsy and MRI. Pathologic result was chronic lobular granulomatous mastitis. (a, b) On axial breast MRI, clustered ring pattern of nonmass enhancement at left breast peripheral portion is seen with diffuse skin thickening and enhancement (arrow). The findings are consistent with microabscess. (c) On sagittal breast MRI, mild skin retraction abutting to microabscess is clearly seen (arrow).
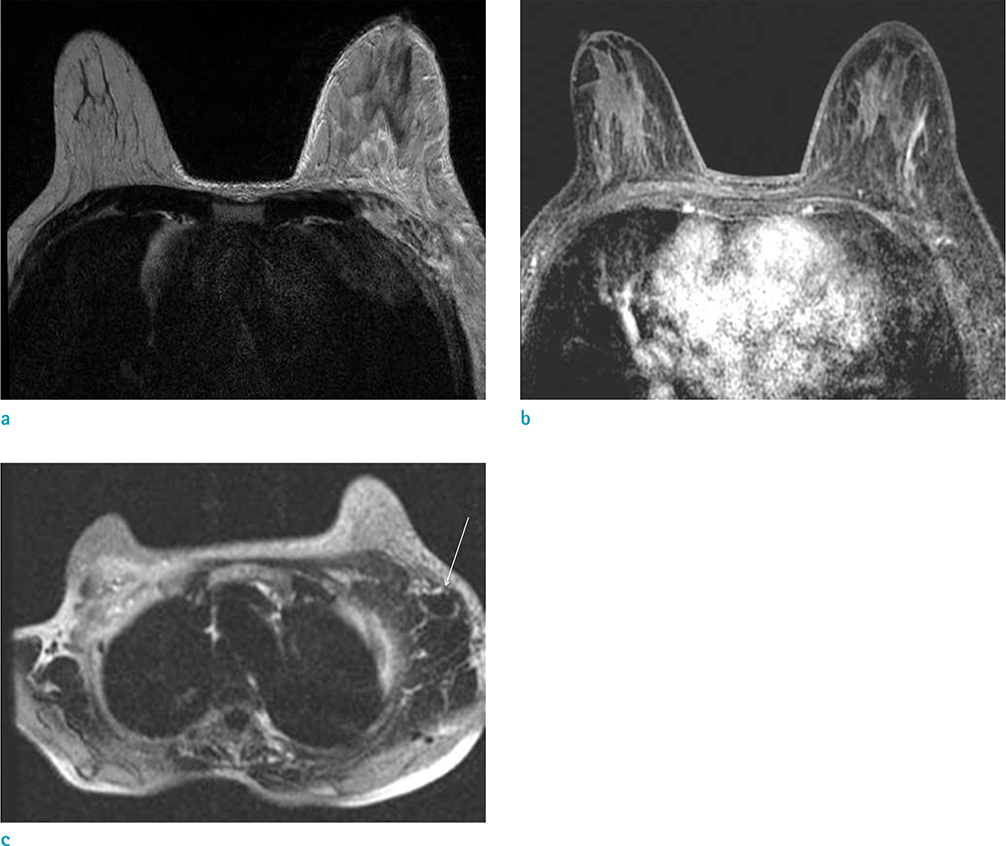
Fig. 16 A 56-year-old woman, who was diagnosed ovarian cancer with metastatic cancer in left axilla, underwent breast MRI. (a, b) On axial T2 and T1 weighted breast MRI, diffuse skin and trabecular thickening of left breast are clearly seen. (c) On axial MRI for axilla, multiple conglomerated metastatic lymph nodes (arrow) are seen. The findings are consistent with obstructive edema due to blocked lymphatics or vein occlusion.
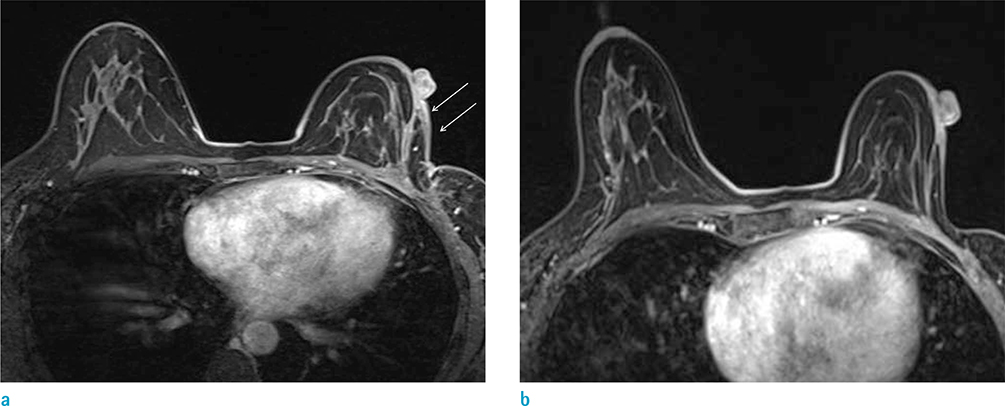
Fig. 17 A 42-year-old woman underwent wide excision of left breast due to invasive ductal cancer. She underwent breast MRI annually after the operation. (a) On axial breast MRI after operation, parenchymal defect with architectural distortion at left breast is seen. Focal skin thickening and enhancement (arrows) is also evident, which is consistent with postoperative and postradiation change. (b) After four years from operation, the skin thickening and enhancement are regressed.
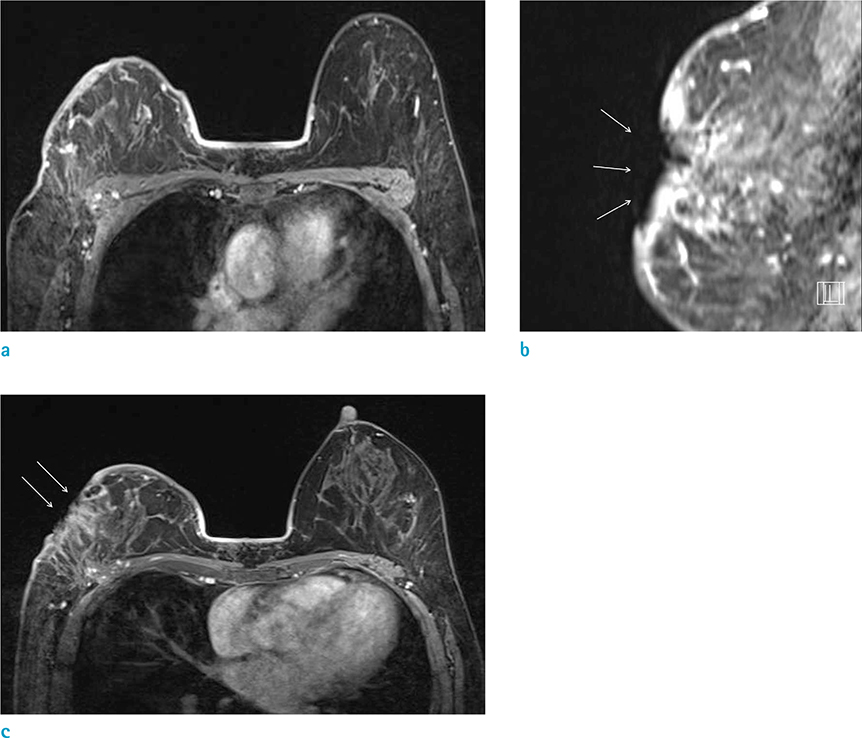
Fig. 18 A 58-year-old woman, who was diagnosed breast cancer 2 years before but refused any treatment at that time, visits outpatient clinic for control growing mass at breast. She underwent combined chemotherapy and radiation therapy on her right breast. During the radiation therapy, she suffered from radiation ulcer. (a) On axial breast MRI nonmass enhancement at outer portion of right breast and diffuse skin thickening with enhancement is seen. (b, c) On axial and sagittal breast MRI, skin defect (arrows) on diffusely thickened breast skin thickening is clearly seen, which is radiation ulcer.
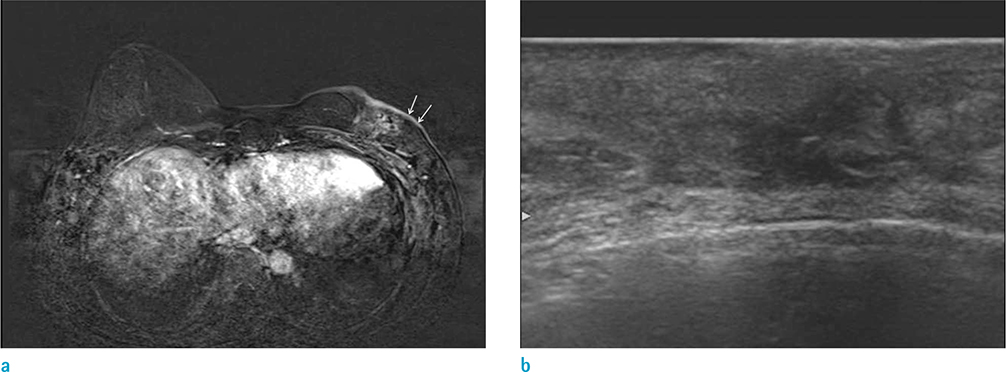
Fig. 19 A 59-year-old woman, who underwent HIFU for treatment of left breast cancer, visited our hospital for evaluation of treatment response. Her skin on breast was burned during the High-intensity focused ultrasound. (a) On axial breast MRI, focal skin thickening with enhancement on her left breast is seen (arrows). (b) On US image, skin thickening overlying irregular hypoechoic lesion (ablated mass) is clearly seen.

Fig. 20 A 47-year-old woman underwent modified radical mastectomy with immediate breast reconstruction with contralateral free DIEP flap coverage due to breast cancer. (a, b) On axial breast MRI, diffuse skin thickening and fat necrosis on reconstructed left breast is evident. (c) On US image, diffuse skin thickening and fat necrosis in reconstructed breast is also seen clearly.
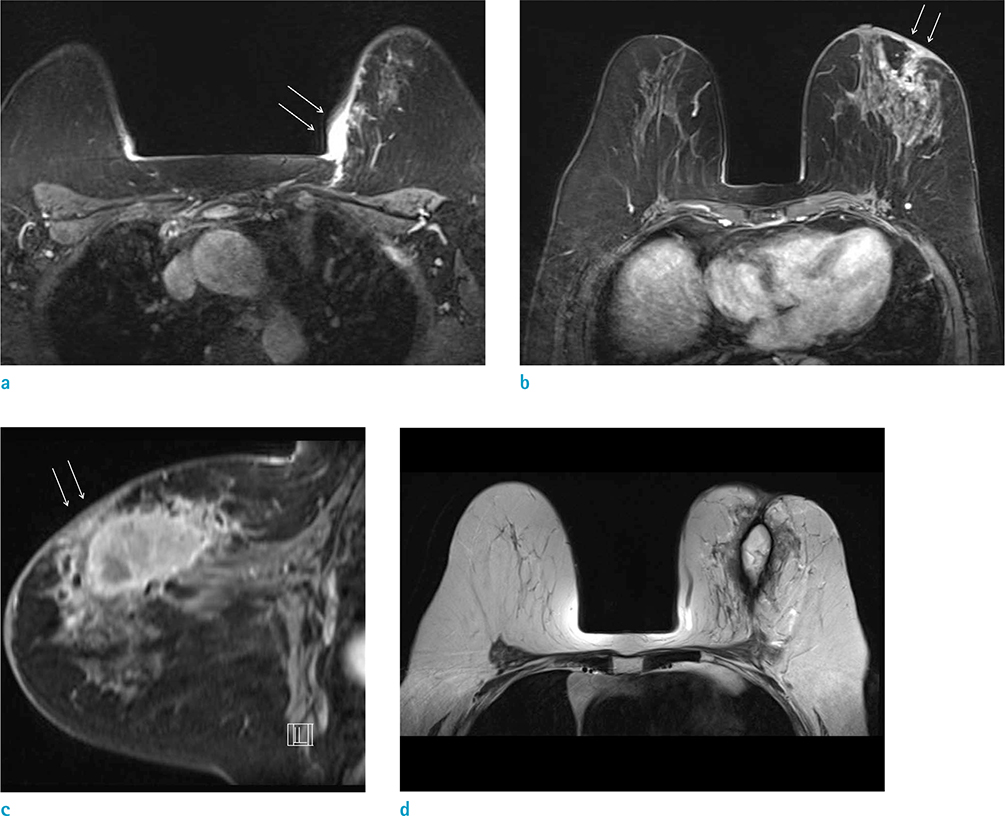
Fig. 21 A 71-year-old woman, who underwent passenger's traffic accident, visited outpatient clinic for evaluation of palpable mass on her left breast. She underwent core needle biopsy for left breast, pathologic result was hematoma formation and fat necrosis due to seat belt injury. (a-c) On axial and sagittal breast MRI, nonenhancing mass at left breast upper portion is seen, suggesting hematoma with fat necrosis. Focal skin thickening with retraction (arrows) and minimal trabecular thickening are also evident. (d) On axial T2 image, high signal intensity hematoma and edema are seen in left breast.
Cited by 1 articles
-
Introduction of a New Staging System of Breast Cancer for Radiologists: An Emphasis on the Prognostic Stage
Jieun Koh, Min Jung Kim
Korean J Radiol. 2019;20(1):69-82. doi: 10.3348/kjr.2018.0231.
Reference
-
1. Kalli S, Freer PE, Rafferty EA. Lesions of the skin and superficial tissue at breast MR imaging. Radiographics. 2010; 30:1891–1913.2. Morris EA, Liberman L. Breast MRI: diagnosis and intervention. 2005; New York, NY: Springer.3. Dershaw DD, Moore MP, Liberman L, Deutch BM. Inflammatory breast carcinoma: mammographic findings. Radiology. 1994; 190:831–834.4. Ellis DL, Teitelbaum SL. Inflammatory carcinoma of the breast. A pathologic definition. Cancer. 1974; 33:1045–1047.5. Yang WT, Le-Petross HT, Macapinlac H, et al. Inflammatory breast cancer: PET/CT, MRI, mammography, and sonography findings. Breast Cancer Res Treat. 2008; 109:417–426.6. Le-Petross HT, Cristofanilli M, Carkaci S, et al. MRI features of inflammatory breast cancer. AJR Am J Roentgenol. 2011; 197:W769–W776.7. Le-Petross CH, Bidaut L, Yang WT. Evolving role of imaging modalities in inflammatory breast cancer. Semin Oncol. 2008; 35:51–63.8. Girardi V, Carbognin G, Camera L, et al. Inflammatory breast carcinoma and locally advanced breast carcinoma: characterisation with MR imaging. Radiol Med. 2011; 116:71–83.9. Anderson WF, Chu KC, Chang S. Inflammatory breast carcinoma and noninflammatory locally advanced breast carcinoma: distinct clinicopathologic entities? J Clin Oncol. 2003; 21:2254–2259.10. Renz DM, Baltzer PA, Bottcher J, et al. Inflammatory breast carcinoma in magnetic resonance imaging: a comparison with locally advanced breast cancer. Acad Radiol. 2008; 15:209–221.11. Haagensen CD, Stout AP. Carcinoma of the breast. II-Criteria of operability. Ann Surg. 1943; 859–870.12. Haagensen CD, Bodian C. A personal experience with Halsted's radical mastectomy. Ann Surg. 1984; 199:143–150.13. Gueth U, Wight E, Schoetzau A, et al. Non-inflammatory skin involvement in breast cancer, histologically proven but without the clinical and histological T4 category features. J Surg Oncol. 2007; 95:291–297.14. Guth U, Singer G, Langer I, et al. T4 category revision enhances the accuracy and significance of stage III breast cancer. Cancer. 2006; 106:2569–2575.15. Guth U, Wight E, Schotzau A, et al. A new approach in breast cancer with non-inflammatory skin involvement. Acta Oncol. 2006; 45:576–583.16. Guth U, Wight E, Singer G. Breast cancer with noninflammatory skin involvement: new data revise the traditional image of a "classical" clinicopathologic entity. Praxis (Bern 1994). 2006; 95:1829–1835.17. Wieland AW, Louwman MW, Voogd AC, van Beek MW, Vreugdenhil G, Roumen RM. Determinants of prognosis in breast cancer patients with tumor involvement of the skin (pT4b). Breast J. 2004; 10:123–128.18. Stavros AT, Rapp CL, Parker SH. Breast ultrasound. 2004; Philadelphia: Lippincott Williams & Wilkins.19. Kamby C, Andersen J, Ejlertsen B, et al. Pattern of spread and progression in relation to the characteristics of the primary tumour in human breast cancer. Acta Oncol. 1991; 30:301–308.20. Orel SG, Fowble BL, Solin LJ, Schultz DJ, Conant EF, Troupin RH. Breast cancer recurrence after lumpectomy and radiation therapy for early-stage disease: prognostic significance of detection method. Radiology. 1993; 188:189–194.21. Ralleigh G, Walker AE, Hall-Craggs MA, Lakhani SR, Saunders C. MR imaging of the skin and nipple of the breast: differentiation between tumour recurrence and post-treatment change. Eur Radiol. 2001; 11:1651–1658.22. Voogd AC, van Tienhoven G, Peterse HL, et al. Local recurrence after breast conservation therapy for early stage breast carcinoma: detection, treatment, and outcome in 266 patients. Dutch Study Group on Local Recurrence after Breast Conservation (BORST). Cancer. 1999; 85:437–446.23. Vaughan A, Dietz JR, Aft R, et al. Scientific Presentation Award. Patterns of local breast cancer recurrence after skin-sparing mastectomy and immediate breast reconstruction. Am J Surg. 2007; 194:438–443.24. Bolin DJ, Lukas GM. Low-grade dermal angiosarcoma of the breast following radiotherapy. Am Surg. 1996; 62:668–672.25. Fineberg S, Rosen PP. Cutaneous angiosarcoma and atypical vascular lesions of the skin and breast after radiation therapy for breast carcinoma. Am J Clin Pathol. 1994; 102:757–763.26. Hunter TB, Martin PC, Dietzen CD, Tyler LT. Angiosarcoma of the breast. Two case reports and a review of the literature. Cancer. 1985; 56:2099–2106.27. Sanders LM, Groves AC, Schaefer S. Cutaneous angiosarcoma of the breast on MRI. AJR Am J Roentgenol. 2006; 187:W143–W146.28. Nouri K. Skin cancer. New York: McGraw-Hill Medical;2008.29. Nebesio CL, Goulet RJ, Jr , Helft PR, Billings SD. Metastatic esophageal carcinoma masquerading as inflammatory breast carcinoma. Int J Dermatol. 2007; 46:303–305.30. Sy AN, Lam TP, Khoo US. Subcutaneous panniculitislike T-cell lymphoma appearing as a breast mass: a difficult and challenging case appearing at an unusual site. J Ultrasound Med. 2005; 24:1453–1460.31. Uematsu T, Kasami M. 3T-MRI, elastography, digital mammography, and FDG-PET CT findings of subcutaneous panniculitis-like T-cell lymphoma (SPTCL) of the breast. Jpn J Radiol. 2012; 30:766–771.32. Shim E, Song SE, Seo BK, Kim YS, Son GS. Lymphoma affecting the breast: a pictorial review of multimodal imaging findings. J Breast Cancer. 2013; 16:254–265.33. Crowe DJ, Helvie MA, Wilson TE. Breast infection. Mammographic and sonographic findings with clinical correlation. Invest Radiol. 1995; 30:582–587.34. Ulitzsch D, Nyman MK, Carlson RA. Breast abscess in lactating women: US-guided treatment. Radiology. 2004; 232:904–909.35. Renz DM, Baltzer PA, Bottcher J, et al. Magnetic resonance imaging of inflammatory breast carcinoma and acute mastitis. A comparative study. Eur Radiol. 2008; 18:2370–2380.36. Fletcher A, Magrath IM, Riddell RH, Talbot IC. Granulomatous mastitis: a report of seven cases. J Clin Pathol. 1982; 35:941–945.37. Han BK, Choe YH, Park JM, et al. Granulomatous mastitis: mammographic and sonographic appearances. AJR Am J Roentgenol. 1999; 173:317–320.38. Van Ongeval C, Schraepen T, Van Steen A, Baert AL, Moerman P. Idiopathic granulomatous mastitis. Eur Radiol. 1997; 7:1010–1012.39. Gautier N, Lalonde L, Tran-Thanh D, et al. Chronic granulomatous mastitis: imaging, pathology and management. Eur J Radiol. 2013; 82:e165–e175.40. Kwak JY, Kim EK, Chung SY, et al. Unilateral breast edema: spectrum of etiologies and imaging appearances. Yonsei Med J. 2005; 46:1–7.41. Heywang-Kobrunner SH, Schlegel A, Beck R, et al. Contrast-enhanced MRI of the breast after limited surgery and radiation therapy. J Comput Assist Tomogr. 1993; 17:891–900.42. Wu F, Wang ZB, Chen WZ, et al. Extracorporeal high intensity focused ultrasound ablation in the treatment of 1038 patients with solid carcinomas in China: an overview. Ultrason Sonochem. 2004; 11:149–154.43. Taboada JL, Stephens TW, Krishnamurthy S, Brandt KR, Whitman GJ. The many faces of fat necrosis in the breast. AJR Am J Roentgenol. 2009; 192:815–825.44. Giess CS, Raza S, Birdwell RL. Distinguishing breast skin lesions from superficial breast parenchymal lesions: diagnostic criteria, imaging characteristics, and pitfalls. Radiographics. 2011; 31:1959–1972.45. Iglesias A, Arias M, Santiago P, Rodriguez M, Manas J, Saborido C. Benign breast lesions that simulate malignancy: magnetic resonance imaging with radiologic-pathologic correlation. Curr Probl Diagn Radiol. 2007; 36:66–82.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Benefit of Sonography in Pregnancy-associated Breast Cancer
- Role of MRI in Diagnostic Evaluation of Papillary Lesions of the Breast
- The Role of Preoperative Breast MRI in Patients With Early-Stage Breast Cancer
- Imaging Diagnosis of Breast Tuberculosis
- Diffusion-Weighted Imaging as a Stand-Alone Breast Imaging Modality
