Primary Multiple Cardiac Myxomas in a Patient without the Carney Complex
- Affiliations
-
- 1Department of Cardiology, Cardiovascular Center, Ogikubo Hospital, Tokyo, Japan. shoheikataoka0818@gmail.com
- KMID: 2161000
- DOI: http://doi.org/10.4250/jcu.2016.24.1.71
Abstract
- Cardiac tumors are rare, and multiple myxomas are even rarer. The latter phenomenon is mostly associated with the Carney complex, a dominantly inherited disease characterized by multiple primary cardiac myxomas, endocrinopathy, and spotty pigmentation of the skin. We report the rare case of a patient who did not have the Carney complex but had multiple primary cardiac tumors. A 78-year-old woman with a past history of breast cancer was referred to our hospital for further examination of multiple cardiac tumors. Echocardiography showed 4 tumors in the left atrium and left ventricle. We could not diagnose them preoperatively and decided to resect them surgically because they were mobile and could have caused embolism and obstruction. The postoperative pathological findings of all 4 tumors were myxomas, although the patient did not meet the diagnostic criteria of the Carney complex. Therefore, a rare case of multiple primary cardiac myxomas was diagnosed.
Keyword
MeSH Terms
Figure
-
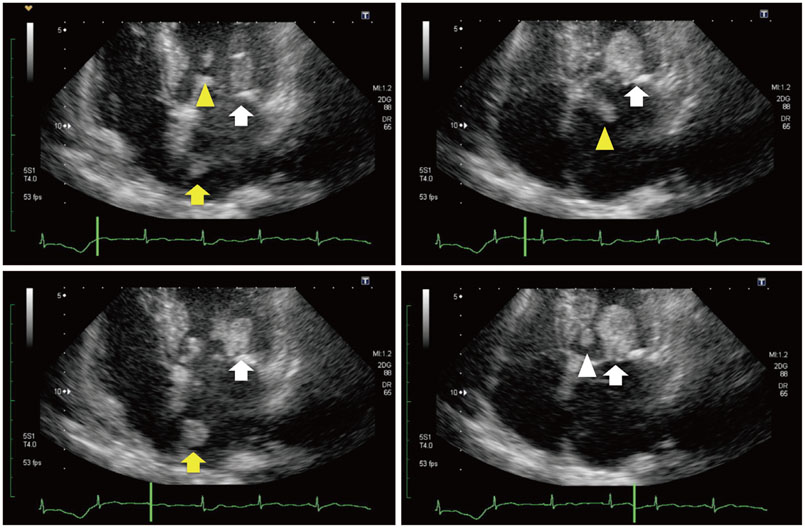
Fig. 1 Transthoracic echocardiography showing 4 masses in the left atrium and left ventricle connected to the interatrial septum (yellow arrows), anterior mitral leaflet (yellow arrowheads), posterior mitral leaflet (white arrows), and aortic valve (white arrowhead).
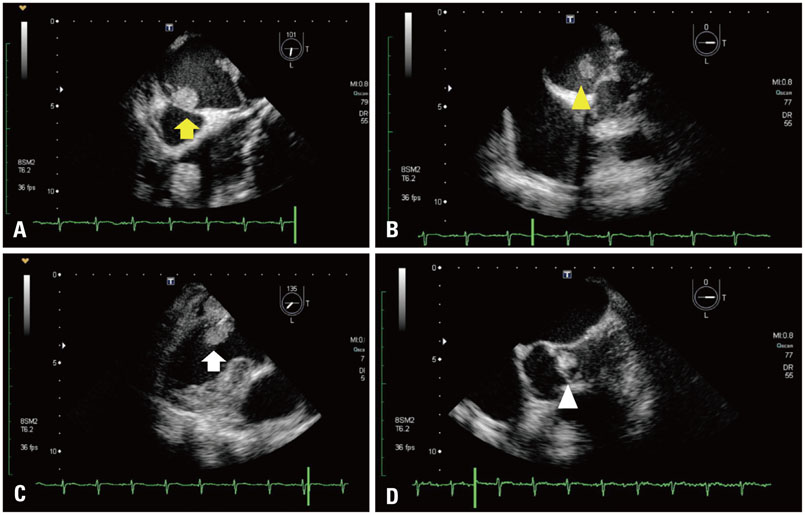
Fig. 2 Transesophageal echocardiography showing the exact position of the 4 tumors. A: An immobile tumor of size 15 × 15 mm at the interatrial septum (yellow arrow). B: A mobile tumor of size 24 × 6 mm (from the left atrium to the left ventricle) at the anterior mitral leaflet (yellow arrowhead). C: An immobile tumor of size 21 × 33 mm at the posterior mitral leaflet (white arrow). D: A mobile tumor of size 11 × 11 mm (from the left ventricular outflow tract to the aorta) at the left leaflet of the aortic valve (white arrowhead).

Fig. 3 Four tumors resected during the operation.
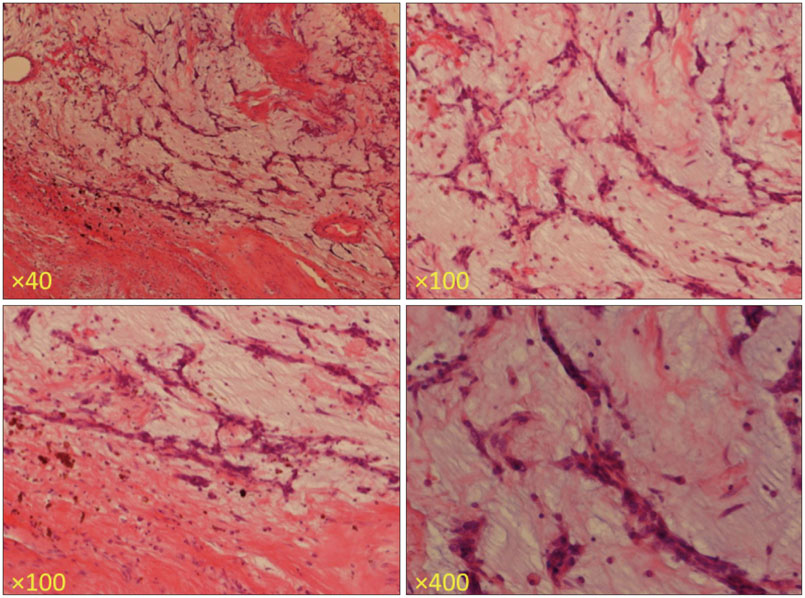
Fig. 4 Histopathological examination showing myxoma cells with a stellate appearance proliferate in a myxoid background in nests and linear syncytia (hematoxylin & eosin staining).
Reference
-
1. Bossert T, Gummert JF, Battellini R, Richter M, Barten M, Walther T, Falk V, Mohr FW. Surgical experience with 77 primary cardiac tumors. Interact Cardiovasc Thorac Surg. 2005; 4:311–315.2. MacGowan SW, Sidhu P, Aherne T, Luke D, Wood AE, Neligan MC, McGovern E. Atrial myxoma: national incidence, diagnosis and surgical management. Ir J Med Sci. 1993; 162:223–226.3. Hoffmeier A, Schmid C, Deiters S, Drees G, Rothenburger M, Tjan TD, Schmidt C, Löher A, Maintz D, Spieker T, Mesters RM, Scheld HH. Neoplastic heart disease -- the Muenster experience with 108 patients. Thorac Cardiovasc Surg. 2005; 53:1–8.4. Raimann A, Wustinger M, Niederle B, Haas O, Häusler G. Cushing, hypertonie, sommersprossen. Der Carney-komplex: fallbericht eines seltenen neoplasiesyndroms. J Clin Endocrinol Metab. 2009; 2:22–25.5. Rahbar K, Seifarth H, Schäfers M, Stegger L, Hoffmeier A, Spieker T, Tiemann K, Maintz D, Scheld HH, Schober O, Weckesser M. Differentiation of malignant and benign cardiac tumors using 18F-FDG PET/CT. J Nucl Med. 2012; 53:856–863.6. Sablotzki A, Welters I, Lehmann N, Menges T, Görlach G, Dehne M, Hempelmann G. Plasma levels of immunoinhibitory cytokines interleukin-10 and transforming growth factor-beta in patients undergoing coronary artery bypass grafting. Eur J Cardiothorac Surg. 1997; 11:763–768.7. Markewitz A, Lante W, Franke A, Marohl K, Kuhlmann WD, Weinhold C. Alterations of cell-mediated immunity following cardiac operations: clinical implications and open questions. Shock. 2001; 16:Suppl 1. 10–15.8. Pinto CA, Marcella S, August DA, Holland B, Kostis JB, Demissie K. Cardiopulmonary bypass has a modest association with cancer progression: a retrospective cohort study. BMC Cancer. 2013; 13:519.9. Canver CC, Marrin CA, Plume SK, Nugent WC. Should a patient with a treated cancer be offered an open heart operation? Ann Thorac Surg. 1993; 55:1202–1204.10. Carrascal Y, Gualis J, Arévalo A, Fulquet E, Flórez S, Rey J, Echevarría JR, Di Stefano S, Fiz L. [Cardiac surgery with extracorporeal circulation in cancer patients: influence on surgical morbidity and mortality and on survival]. Rev Esp Cardiol. 2008; 61:369–375.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Carney Complex: Diagnosed 11 Years after Resection of Recurrent Cardiac Myxomas
- Carney Complex in Three First-Degree Relatives
- A Case of Carney Complex
- Anesthetic experiences of myxoma removal surgery in two patients with Carney complex: A report of two cases
- Carney Complex with Multiple Intracranial Aneurysms
