Cauda Equina Syndrome Caused by Pseudogout Involving the Lumbar Intervertebral Disc
- Affiliations
-
- 1Department of Neurosurgery Dongguk University Ilsan Hospital, Goyang, Korea. ktcho21@naver.com
- 2Department of Pathology, Dongguk University Ilsan Hospital, Goyang, Korea.
- KMID: 2157988
- DOI: http://doi.org/10.3346/jkms.2012.27.12.1591
Abstract
- Calcium pyrophosphate dihydrate (CPPD) deposition disease, also known as pseudogout, is a disease that causes inflammatory arthropathy in peripheral joints, however, symptomatic involvement of the intervertebral disc is uncommon. Herein, we describe a 59-yr-old patient who presented with cauda equina syndrome. Magnetic resonance imaging of the patient showed an epidural mass-like lesion at the disc space of L4-L5, which was compressing the thecal sac. Biopsy of the intervertebral disc and epidural mass-like lesion was determined to be CPPD deposits. We reviewed previously reported cases of pseudogout involving the lumbar intervertebral disc and discuss the pathogenesis and treatment of the disease.
MeSH Terms
Figure
-

Fig. 1 Magnetic resonance imaging and computed tomography of the lumbar spine. (A) A T2-weighted sagittal image shows an epidural mass with heterogeneous signal intensity and the thecal sac is severely compressed by the mass. Focal low density (black arrows) in the lesion is suggestive of calcification. (B) Non-contrast and (C) contrast T1-sagittal image show enhancement (white arrows) in adjacent to the posterior longitudinal ligament. (D) Non-contrast T2- and (E) T1-weighted axial image show the thecal sac is severely compressed by the mass. (F) Computed tomography shows sparse calcification.
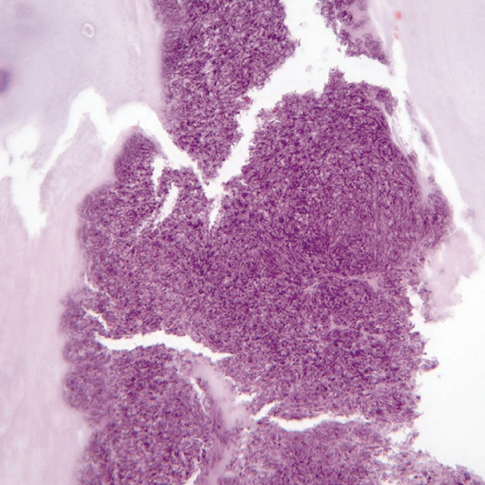
Fig. 2 Histopathologic study of the intervertebral disc and epidural mass-like lesion. Irregular crystalline deposits of calcium pyrophosphate dihydrate are present in the intervertebral disc and epidural mass-like lesion (H&E stain, × 40).
Reference
-
1. Lam HY, Cheung KY, Law SW, Fung KY. Crystal arthropathy of the lumbar spine: a report of 4 cases. J Orthop Surg (Hong Kong). 2007. 15:94–101.2. Jeon CH, Choe WH, Ahn JK, Koh JH, Cha HS, Ahn JM, Koh EM. Calcium Pyrophosphate Dihydrate (CPPD) Crystal Deposition Disease Mimicking Meningitis: a case report and review of the literature. J Korean Rheum Assoc. 2001. 8:134–139.3. Andres TL, Trainer TD. Intervertebral chondrocalcinosis: a coincidental finding possibly related to previous surgery. Arch Pathol Lab Med. 1980. 104:269–271.4. Delamarter RB, Sherman JE, Carr J. Lumbar spinal stenosis secondary to calcium pyrophosphate crystal deposition (pseudogout). Clin Orthop Relat Res. 1993. 289:127–130.5. Salcman M, Khan A, Symonds DA. Calcium pyrophosphate arthropathy of the spine: case report and review of the literature. Neurosurgery. 1994. 34:915–918.6. Abhishek A, Doherty M. Pathophysiology of articular chondrocalcinosis--role of ANKH. Nat Rev Rheumatol. 2011. 7:96–104.7. Baty V, Prost B, Jouvet A, Laurent J, Vallée B. Acute spinal cord compression and calcium pyrophosphate deposition disease. Case illustration. J Neurosurg. 2003. 99:2 Suppl. 240.8. Richards AJ, Hamilton EB. Spinal changes in idiopathic chondrocalcinosis articularis. Rheumatol Rehabil. 1976. 15:138–142.9. Bywaters EG, Hamilton EB, Williams R. The spine in idiopathic haemochromatosis. Ann Rheum Dis. 1971. 30:453–465.10. Lagier R, Wildi E. Incidence of chondrocalcinosis in a series of 1,000 surgically excised intervertebral disks. Rev Rhum Mal Osteoartic. 1979. 46:303–307.11. Mohr W, Oehler K, Hersener J, Wilke W. Chondrocalcinosis of the intervertebral disks. Z Rheumatol. 1979. 38:11–26.12. Berlemann U, Gries NC, Moore RJ, Fraser RD, Vernon-Roberts B. Calcium pyrophosphate dihydrate deposition in degenerate lumbar discs. Eur Spine J. 1998. 7:45–49.13. Ellman MH, Vazques LT, Brown NL, Mandel N. Calcium pyrophosphate dihydrate deposition in lumbar disc fibrocartilage. J Rheumatol. 1981. 8:955–958.14. Doita M, Shimomura T, Maeno K, Nishida K, Fujioka H, Kurosaka M. Calcium pyrophosphate dihydrate deposition in the transverse ligament of the atlas: an unusual cause of cervical myelopathy. Skeletal Radiol. 2007. 36:699–702.15. Muthukumar N, Karuppaswamy U. Tumoral calcium pyrophosphate dihydrate deposition disease of the ligamentum flavum. Neurosurgery. 2003. 53:103–108.16. Brown TR, Quinn SF, D'Agostino AN. Deposition of calcium pyrophosphate dihydrate crystals in the ligamentum flavum: evaluation with MR imaging and CT. Radiology. 1991. 178:871–873.17. Zhang W, Doherty M, Pascual E, Barskova V, Guerne PA, Jansen TL, Leeb BF, Perez-Ruiz F, Pimentao J, Punzi L, et al. EULAR recommendations for calcium pyrophosphate deposition. Part II: management. Ann Rheum Dis. 2011. 70:571–575.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Posterior Epidural Migration of a Sequestrated Intervertebral lumbar Disc with Cauda Equina Syndrome: Two Cases Report
- Sudden Onset of Cauda Equina Syndrome Resulting from Posterior Migration of Lumbar Herniated Disc Without Significant Previous Neurological Signs
- Dorsally Migrated Sequestrated Lumbar Disc Herniation with Cauda Equina Syndrome: Two Cases Report
- A Case of Posterior Epidural Migration of an Extruded Lumbar Disc Fragment Causing Cauda Equina Syndrome
- Ruptured Lumbar Disc in Patients Undergoing Manipulation of the Lumbar Spine
