Radiofrequency Neurotomy of Cervical Medial Branches for Chronic Cervicobrachialgia
- Affiliations
-
- 1Department of Neurosurgery, Presbyterian Medical Center, Jeonju, Korea. hyoungihl@hotmail.com
- KMID: 2157794
- DOI: http://doi.org/10.3346/jkms.2006.21.1.119
Abstract
- Chronic neck and arm pain or cervicobrachialgia commonly occurs with the degeneration of cervical spine. Authors investigated the usefulness of radiofrequency (RF) neurotomies of cervical medial branches in patients with cervicobrachialgia and analyzed the factors which can influence the treatment outcome. Demographic data, types of pain distribution, responses of double controlled blocks, electrical stimulation parameters, numbers and levels of neurotomies, and surgical outcomes were evaluated after mean follow-up of 12 months. Pain distribution pattern was not significantly correlated with the results of diagnostic blocks. Average stimulation intensity was 0.45 V, ranging from 0.3 to 0.69, to elicit pain response in cervical medial branches. The most common involvement of nerve branches was C4 (89%), followed by C5 (82%), C6 (75%), and C7 (43%). Among total of 28 patients, nineteen (68%) reported successful outcome according to outcome criteria after 6 months of followup (p=0.001), and eight (42%) of 19 patients reported complete relief (100%) of pain. Four patients showed recurrence of pain between 6 and 12 months. It was therefore concluded that cervical medial branch neurotomy is considered useful therapeutic modality for the management of cervicobrachialgia in selected patients, particularly in degenerative zygapophyseal disorders.
Keyword
MeSH Terms
-
Adult
Aged
Aged, 80 and over
Back Pain/etiology/surgery
Brachial Plexus/pathology/*surgery
Brachial Plexus Neuritis/complications/diagnosis/*surgery
Chronic Disease
Electrosurgery/methods
Female
Humans
Male
Middle Aged
Neck Pain/etiology/surgery
Nerve Block/methods
Neurosurgical Procedures/instrumentation/*methods
Treatment Outcome
Figure
-
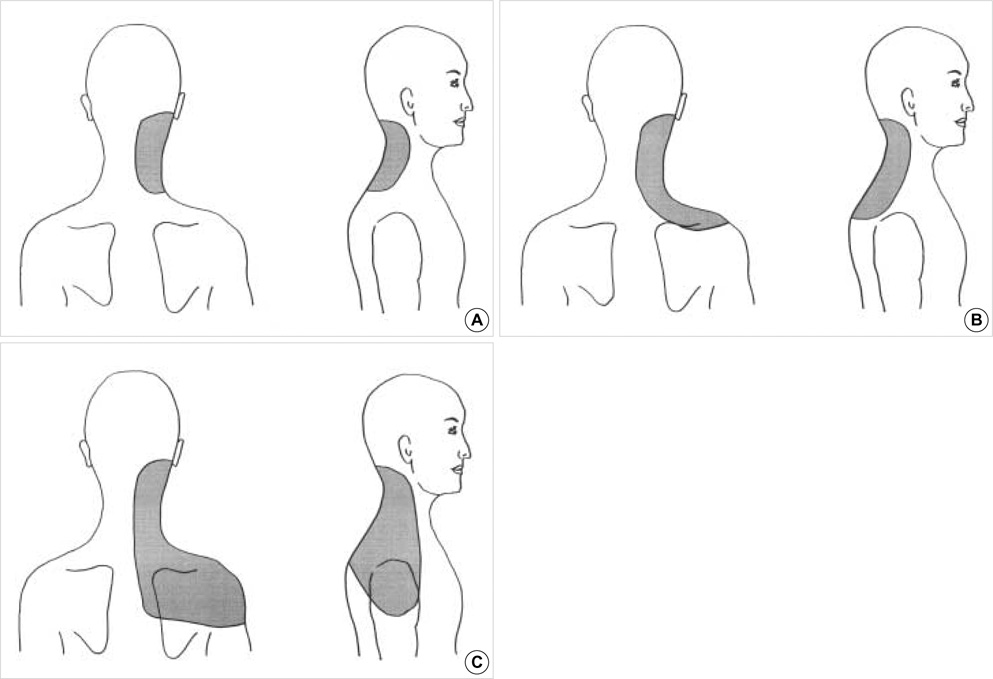
Fig. 1 Pain distribution patterns in the patients with degenerative cervical spine. Type A denotes the pain distribution in the lower neck (A); type B demonstrates the pain in the neck and shoulder (B); type C indicates the pain in lower neck, shoulder, sometimes scapula, and upper arm (C).

Fig. 2 Radiograph of cervical spine anteroposterior (A) and lateral view (B) demonstrating the location of needles for nerve blocks branches performed on C4, C5, C6 and C7 medial branches.
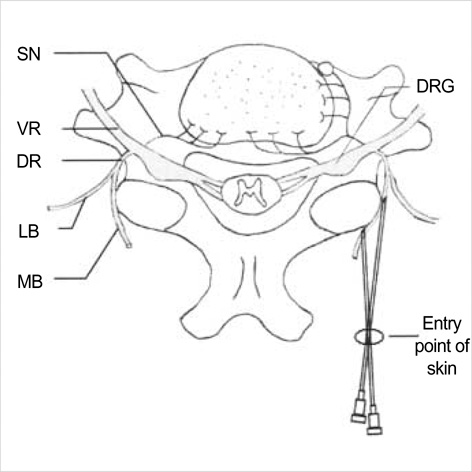
Fig. 3 Schematic drawing demonstrating the targets of radiofrequency neurotomy of cervical medial branch. VR, ventral ramus; DR, dorsal ramus; LB, lateral branch; MB, medial branch; DRG, dorsal root ganglion; SN, sinuvertebral nerve.
Cited by 2 articles
-
Diagnostic Relevance of Pressure-Controlled Discography
Dong-Ah Shin, Hyoung-Ihl Kim, Jae-Hyun Jung, Dong-Gyu Shin, Jung-Ok Lee
J Korean Med Sci. 2006;21(5):911-916. doi: 10.3346/jkms.2006.21.5.911.Nonoperative interventions for spinal pain
Dong Ah Shin, Hyoung Ihl Kim
J Korean Med Assoc. 2014;57(4):308-317. doi: 10.5124/jkma.2014.57.4.308.
Reference
-
1. Guez M, Hildingsson C, Nilson M, Toolanen G. The prevalence of neck pain: a population-based study from northern Sweden. Acta Orthop Scand. 2002. 73:455–459.2. Manchikanti L. Facet joint pain and the role of neural blockade in its management. Curr Rev Pain. 1999. 3:348–358.
Article3. Joy H, Ha SK, Kim SH, Lim DJ, Park JY, Suh JK. Prognostic factors of percutaneous radiofrequency neurotomy of posterior primary ramus. J Korean Neurosurg Soc. 2003. 33:51–55.4. Schellhas KP. Facet nerve blockade and radiofrequency neurotomy. Neuroimaging Clin N Am. 2000. 10:493–501.5. Schwartzer AC, Aprill CN, Derby R, Fortin J, Kine J, Bogduk N. The false-positive rate of uncontrolled diagnostic blocks of the lumbar zygapophysial joints. Pain. 1994. 58:195–200.6. Tzaan WC, Tasker RR. Percutaneous radiofrequency facet rhizotomy: experience with 118 procedures and reappraisal of its value. Can J Neurol Sci. 2000. 27:125–130.7. Aprill C, Bogduk N. The prevalence of cervical zygapophyseal joint pain: a first approximation. Spine. 1992. 17:744–747.
Article8. Lord SM, Barnsley L, Bogduk N. Percutaneous radiofrequency neurotomy in the treatment of cervical zygapophysial joint pain: a caution. Neurosurgery. 1995. 36:732–739.9. Lord SM, Barnsley L, Wallis BJ, McDonald GJ, Bogduk N. Percutaneous radio-frequency neurotomy for chronic cervical zygapophyseal joint pain. N Engl J Med. 1996. 335:1721–1726.10. Barnsley L, Lord S, Wallis B, Bogduk N. The prevalence of chronic cervical zygapophysial joint pain after whiplash. Spine. 1995. 20:20–26.
Article11. Schaerer JP. Radiofrequency facet rhizotomy in the treatment of chronic neck and low back pain. Int Surg. 1978. 63:53–59.12. Slujiter ME, Koetsveld-Baart CC. Interruption of pain pathways in the treatment of the cervicogenic syndrome. Anesthesia. 1980. 35:302–307.13. Hildebrant J, Argyrakis A. Percutaneous nerve block of the cervical facets: a relatively new method in the treatment of chronic headache and neck pain. Man Med. 1986. 2:48–52.14. Vervest AC, Stolker RJ. The treatment of cervical pain syndrome with radiofrequency procedures. Pain Clinic. 1991. 4:103–112.15. Kim HI, Shin DG, Shin DA, Lee JO. Pain evaluation for decision making for management of spinal pain. J Korean Soc Stereotax Func Neurosurg. 2005. 1:44–50.16. Rao R. Neck pain, cervical radiculopathy, and cervical myelopathy: pathophysiology, natural history, and clinical evaluation. J Bone Joint Surg Am. 2002. 84-A:1872–1881.17. Gore DR, Sepic SB, Gardner GM. Roentgenographic findings of the cervical spine in asymptomatic people. Spine. 1986. 11:521–524.
Article18. Heller CA, Stanley P, Lewis-Jones B, Heller RF. Value of x-ray examinations of the cervical spine. Br Med J. 1983. 287:1276–1279.19. Boos N, Rieder R, Schade V, Spratt KF, Semmer N, Aebi M. The diagnostic accuracy of magnetic resonance imaging, work perception, and psychosocial factors in identifying symptomatic disc herniations. Spine. 1995. 20:2613–2625.
Article20. Bogduk N, Marsland A. The cervical zygapophysial joints as a source of neck pain. Spine. 1988. 13:610–617.
Article21. Barnsley L, Lord S, Wallis B, Bogduk N. False positive rates of cervical zygapophysial joint blocks. Clin J Pain. 1993. 9:124–130.22. Schwarzer AC, Wang SC, O'Driscoll D, Harrington T, Bogduk N, Laurent R. The ability of computed tomography to identify a painful zygapophysial joint in patients with chronic low back pain. Spine. 1995. 20:907–912.
Article23. Spitzer WO, Skovron ML, Salmi LR, Cassidy JD, Duranceau J, Suissa S, Zeiss E. Scientific monograph of the Quebec Task Force on Whiplash-Associated Disorders: redefining "whiplash" and its management. Spine. 1995. 20:Suppl. 1–73.24. Barnsley L, Bogduk N. Medial branch blocks are specific for the diagnosis of cervical zygapophysial joint pain. Reg Anesth. 1993. 18:343–350.25. Barnsley L, Lord S, Bogduk N. Comparative local anaesthetic blocks in the diagnosis of cervical zygapophysial joints pain. Pain. 1993. 55:99–106.26. McDonald G, Lord SM, Bogduk N. Long-term follow-up of patients treated with cervical radiofrequency neurotomy for chronic neck pain. Neurosurgery. 1999. 45:61–67.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Effect of Radiofrequency Neurotomy of Lower Cervical Medial Branches on Cervicogenic Headache
- New More Reliable Indicator for Confirmation of the Medial Branch in Radiofrequency Neurotomy
- Interventional Treatment for Cervical Pain
- Radiofrequency Neurotomy of the Medial Branch for the Management of Lumbar Zygapophysial Joint Pain
- Burn Wound along the Guide Needle Trajectory as a Complication of Radiofrequency Neurotomy of the Lumbar Medial Branch: A case report
