Neurointervention.
2016 Mar;11(1):37-41. 10.5469/neuroint.2016.11.1.37.
Outpatient Day-care Neuroangiography and Neurointervention of Unruptured Intracranial Aneurysms
- Affiliations
-
- 1Departments of Radiology and Research Institute of Radiology, University of Ulsan, College of Medicine, Asan Medical Center, Seoul, Korea. dcsuh@amc.seoul.kr
- 2Department of Interventional Radiology, Taizhou People's Hospital, Taizhou, Jiangsu Province 225300, P. R. China.
- KMID: 2155717
- DOI: http://doi.org/10.5469/neuroint.2016.11.1.37
Abstract
- PURPOSE
Day-care management of unruptured intracranial aneurysms can shorten hospital stay, reduce medical cost and improve outcome. We present the process, outcome and duration of hospital stay for the management of unruptured intracranial aneurysms via a neurointervention clinic in a single center during the past four years.
MATERIALS AND METHODS
We analyzed 403 patients who were referred to Neurointervention Clinic at Asan Medical Center for aneurysm evaluation between January 1, 2011 and December 31, 2014. There were 141 (41%) diagnostic catheter angiographies, 202 (59%) neurointerventional procedures and 2 (0.6%) neurointerventional procedures followed by operation. We analyzed the process, outcome of angiography or neurointervention, and duration of hospital stay.
RESULTS
There was no aneurysm in 58 patients who were reported as having an aneurysm in MRA or CTA (14 %). Among 345 patients with aneurysm, there were 283 patients with a single aneurysm (82%) and 62 patients with multiple aneurysms (n=62, 18%). Aneurysm coiling was performed in 202 patients (59%), surgical clipping in 14 patients (4%), coiling followed by clipping in 2 patients (0.6%) and no intervention was required in 127 patients (37%). The hospital stay for diagnostic angiography was less than 6 hours and the mean duration of hospital stay was 2.1 days for neurointervention. There were 4 procedure-related adverse events (2%) including 3 minor and 1 major ischemic strokes.
CONCLUSION
Our study revealed that day-care management of unruptured intracranial aneurysms could be performed without an additional risk. It could enable rapid patient flow, shorten hospital stay and thus reduce hospital costs.
MeSH Terms
Figure
-
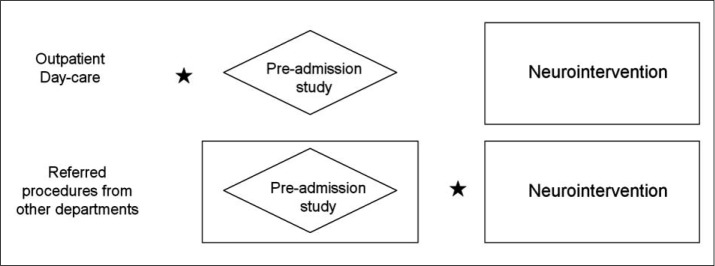
Fig. 1 Process diagram of patient flow. Comparison between outpatient daycare and referred procedures. Preadmission study = chest PA, Electrocardiography (ECG), blood test and urine analysis; ★ = consultation for neurointervention; ◇ = Pre-admission study; ⬜ = Admission status
Reference
-
1. Rinkel GJ. Natural history, epidemiology and screening of unruptured intracranial aneurysms. J Neuroradiol. 2008; 35:99–103. PMID: 18242707.
Article2. Rinkel GJ, Djibuti M, Algra A, van Gijn J. Prevalence and risk of rupture of intracranial aneurysms: a systematic review. Stroke. 1998; 29:251–256. PMID: 9445359.3. UCAS Japan Investigators. Morita A, Kirino T, Hashi K, Aoki N, Fukuhara S, et al. The natural course of unruptured cerebral aneurysms in a Japanese cohort. N Engl J Med. 2012; 366:2474–2482. PMID: 22738097.
Article4. Juvela S, Porras M, Poussa K. Natural history of unruptured intracranial aneurysms: probability of and risk factors for aneurysm rupture. J Neurosurg. 2008; 108:1052–1060. PMID: 18447733.
Article5. You SH, Kong DS, Kim JS, Jeon P, Kim KH, Roh HK, et al. Characteristic features of unruptured intracranial aneurysms: predictive risk factors for aneurysm rupture. J Neurol Neurosurg Psychiatry. 2010; 81:479–484. PMID: 19726404.
Article6. Jeon JS, Ahn JH, Huh W, Son YJ, Bang JS, Kang HS, et al. A retrospective analysis on the natural history of incidental small paraclinoid unruptured aneurysm. J Neurol Neurosurg Psychiatry. 2014; 85:289–294. PMID: 23781005.
Article7. Nagamine Y. Natural history and management of asymptomatic unruptured cerebral aneurysms. Rinsho Shinkeigaku. 2004; 44:763–766. PMID: 15651285.8. Unruptured intracranial aneurysms--risk of rupture and risks of surgical intervention. International Study of Unruptured Intracranial Aneurysms Investigators. N Engl J Med. 1998; 339:1725–1173. PMID: 9867550.9. Yoshimoto Y, Tanaka Y. Risk perception of unruptured intracranial aneurysms. Acta Neurochir (Wien). 2013; 155:2029–2203. PMID: 23921577.
Article10. Buijs JE, Greebe P, Rinkel GJ. Quality of life, anxiety, and depression in patients with an unruptured intracranial aneurysm with or without aneurysm occlusion. Neurosurgery. 2012; 70:868–872. PMID: 21937934.
Article11. King JT Jr, Tsevat J, Roberts MS. Preference-based quality of life in patients with cerebral aneurysms. Stroke. 2005; 36:303–330. PMID: 15653579.
Article12. Yamashiro S, Nishi T, Koga K, Goto T, Kaji M, Muta D, et al. Improvement of quality of life in patients surgically treated for asymptomatic unruptured intracranial aneurysms. J Neurol Neurosurg Psychiatry. 2007; 78:497–500. PMID: 17178825.
Article13. McDonald JS, McDonald RJ, Fan J, Kallmes DF, Lanzino G, Cloft HJ. Comparative effectiveness of unruptured cerebral aneurysm therapies: propensity score analysis of clipping versus coiling. Stroke. 2013; 44:988–994. PMID: 23449260.14. Hwang JS, Hyun MK, Lee HJ, Choi JE, Kim JH, Lee NR, et al. Endovascular coiling versus neurosurgical clipping in patients with unruptured intracranial aneurysm: a systematic review. BMC Neurol. 2012; 12:99. PMID: 22998483.
Article15. Brinjikji W, Rabinstein AA, Nasr DM, Lanzino G, Kallmes DF, Cloft HJ. Better outcomes with treatment by coiling relative to clipping of unruptured intracranial aneurysms in the United States, 2001-2008. AJNR Am J Neuroradiol. 2011; 32:1071–1075. PMID: 21511860.
Article16. Jeong YG, Kim EH, Hwang SM, Lee GY, Kim JW, Choi YJ, et al. Outpatient (Same-day care) Neuroangiography and Neurointervention. Neurointervention. 2012; 7:17–22. PMID: 22454780.
Article17. Lu PH, Park JW, Park S, Kim JL, Lee DH, Kwon SU, et al. Intracranial stenting of subacute symptomatic atherosclerotic occlusion versus stenosis. Stroke. 2011; 42:3470–3476. PMID: 21940974.
Article18. Suh DC, Kim JK, Choi JW, Choi BS, Pyun HW, Choi YJ, et al. Intracranial stenting of severe symptomatic intracranial stenosis: results of 100 consecutive patients. AJNR Am J Neuroradiol. 2008; 29:781–785. PMID: 18310234.
Article19. Kwon SC, Kwon OK. Korean Unruptured Cerebral Aneurysm Coiling Investigators. Endovascular coil embolization of unruptured intracranial aneurysms: a Korean multicenter study. Acta Neurochir (Wien). 2014; 156:847–885. PMID: 24610449.
Article20. Naggara ON, Lecler A, Oppenheim C, Meder JF, Raymond J. Endovascular treatment of intracranial unruptured aneurysms: a systematic review of the literature on safety with emphasis on subgroup analyses. Radiology. 2012; 263:828–835. PMID: 22623696.
Article21. Yue W. Endovascular treatment of unruptured intracranial aneurysms. Interv Neuroradiol. 2011; 17:420–424. PMID: 22192544.
Article22. Hoh BL, Chi YY, Dermott MA, Lipori PJ, Lewis SB. The effect of coiling versus clipping of ruptured and unruptured cerebral aneurysms on length of stay, hospital cost, hospital reimbursement, and surgeon reimbursement at the university of Florida. Neurosurgery. 2009; 64:614–619. PMID: 19197221.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Guideline for Management of Unruptured Intracranial Aneurysms: Preliminary Report
- Current Update on the Randomized Controlled Trials of Intracranial Aneurysms
- Surgical Treatment of Unruptured Cerebral Aneurysms
- Outpatient Day-Care Management of Unruptured Intracranial Aneurysm: A Retrospective Cohort Study
- Comprehension of Two Modalities: Endovascular Coiling and Microsurgical Clipping in Treatment of Intracranial Aneurysms
