Interventional Radiological Treatment of Renal Transplant Complications: A Pictorial Review
- Affiliations
-
- 1Department of Radiological Sciences, Institute of Radiology, "A. Gemelli" Hospital - Catholic University, Rome 00168, Italy. roberto.iezzi.md@gmail.com
- 2Department of Surgical Science, Renal Transplantation Unit, "A. Gemelli" Hospital - Catholic University, Rome 00168, Italy.
- KMID: 2155529
- DOI: http://doi.org/10.3348/kjr.2015.16.3.593
Abstract
- Renal transplantation is the treatment of choice for patients with chronic renal failure, which produces a dramatic improvement in the quality of life and survival rates, in comparison to long-term dialysis. Nowadays, new imaging modalities allow early diagnosis of complications, and thanks to the recent developments of interventional techniques, surgery may be avoided in most cases. Knowledge in the types of renal transplant complications is fundamental for a correct pre-operative planning. In this article, we described the most common or clinically relevant renal transplant complications and explained their interventional management.
MeSH Terms
Figure
-
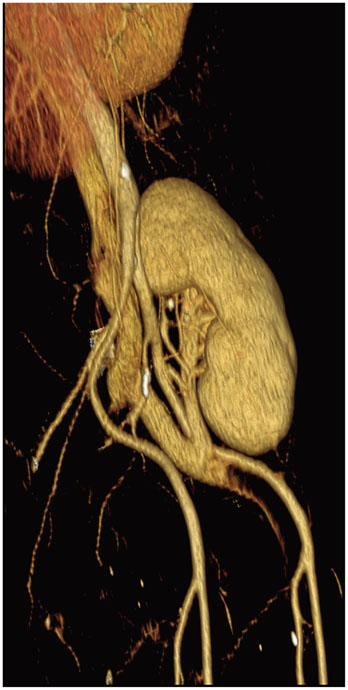
Fig. 1 Volume-rendered image of transplantation kidney shows end-to-side anastomosis between donor renal artery and recipient external iliac artery.
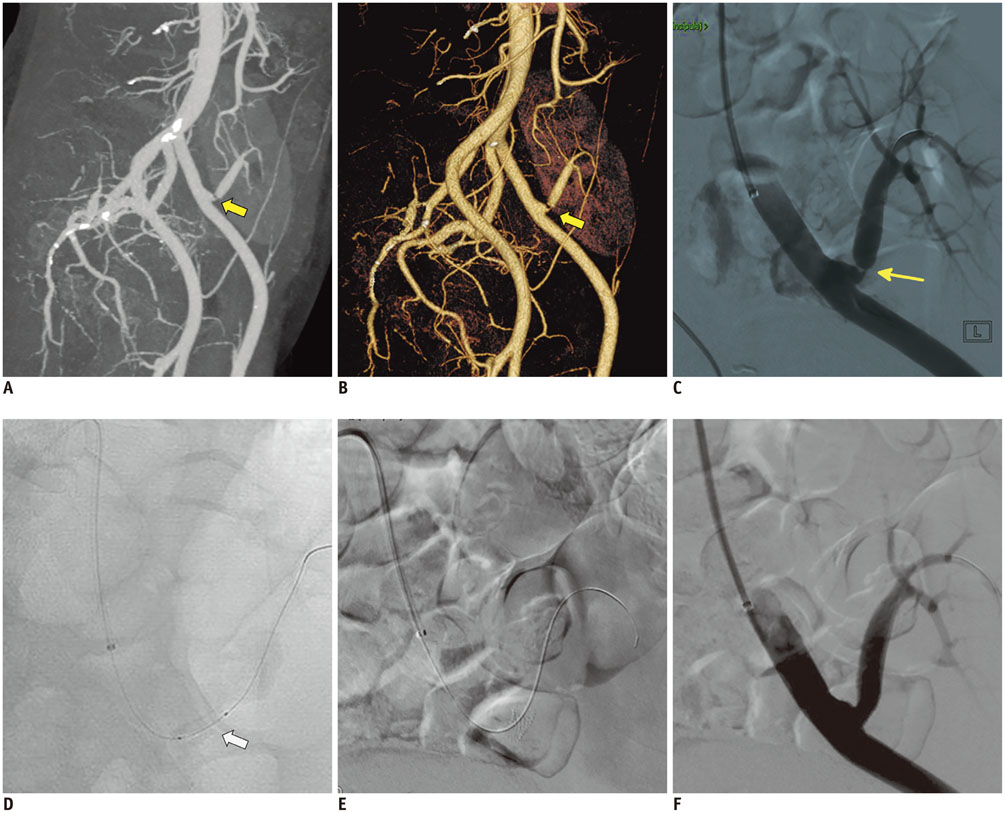
Fig. 2 67-year-old male, who received transplant 3 years before, is presented. A, B. Maximum intensity projection and volume rendered CT images demonstrate severe renal artery end-to-side anastomotic stenosis (arrows). C-F. DSA images: ipsilateral approach is usually preferred to access end-to-side anastomosis with internal iliac artery (as in this patient), whereas contra-lateral approach is usually best for accessing end-to-side anastomosis with external iliac artery. DSA image confirms presence of severe stenosis at site of anastomosis (arrow in C). PTA procedure was performed with successful restoration of renal artery lumen (arrow in D) and final deployment of mono-rail pre-mounted balloon-expandable stent (5 × 18 mm; Tsunami, Terumo, BTG), with minimal residual stenosis. Stent should be used in patients with persistent systolic pressure gradient that exceeds 10 mm Hg after PTA, in case of flow-limiting dissection or residual stenosis > 30%. Pre-mounted balloon-expandable stents are preferred, which maximize deployment position and stability. DSA = digital subtraction angiography, PTA = percutaneous transluminal angioplasty

Fig. 3 50-year-old female is shown, 2 days after transplantation. A, B. Duplex ultrasound images show tardus and parvus waveform in intra-parenchymal renal arteries, with increased velocity and turbulence in main transplant renal artery. C. Three-dimensional MIP reformatted image demonstrates kinking (arrow) of transplanted renal artery. MIP = maximum intensity projection

Fig. 4 33-year-old female with previous left renal graft explantation. A, B. MIP and VR reformatted images illustrate large extrarenal pseudoaneurysm arising at site of previous end-to-end anastomosis, as confirmed by digital subtraction angiography images (arrows). C-E. Successful endovascular treatment was performed, by placing iliac covered stent-graft. MIP = maximum intensity projection, VR = volume-rendered

Fig. 5 47-year-old female is shown, at 1 day after transplantation with two renal arteries anastomosed to external iliac artery. A, B. Three dimensional volume-rendered and maximum intensity projection reformatted images show post-surgery dissection (arrows) of left external iliac artery extending below 2 transplanted renal arteries, both originating from true lumen. C. CT findings were confirmed by digital subtraction angiography (arrow). D-H. Premounted stent (Express, Boston Scientific, USA) was deployed in proximal intimal flap, in order to allow expansion of true lumen and consequent collapsing and exclusion of false lumen.
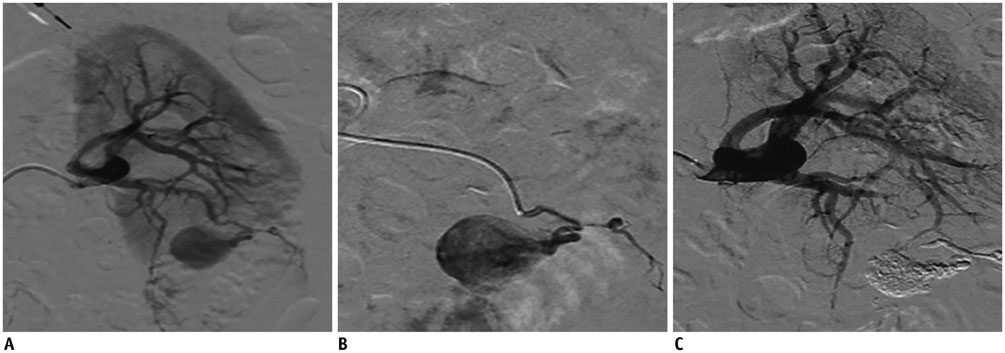
Fig. 6 40-year-old male is shown. A. Selective angiogram of renal artery demonstrates large post-biopsy intra-renal pseudoaneurysm. B, C. After super-selective catheterization, embolization with 33% solution of N-butil cyanoacrylate glue (Glubran 2 + Lipiodol; 1:3, 1 mL) was performed, with complete deafferentation of pseudoaneurysm without any complications or non-target complications.
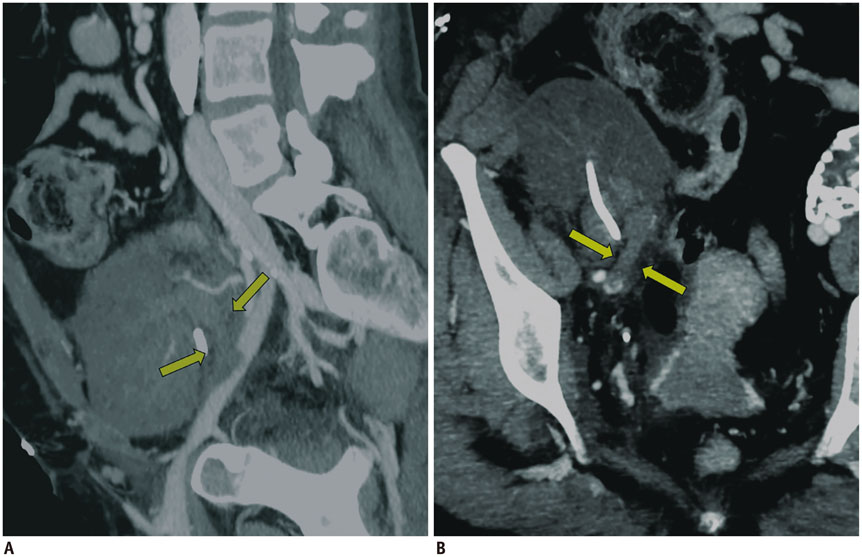
Fig. 7 48-year-old female is shown, at 2 days after transplantation. A, B. Reformatted maximum intensity projection images show thrombosis of transplanted renal vein extending into external iliac vein (arrows), with markedly altered nephrogram of graft.
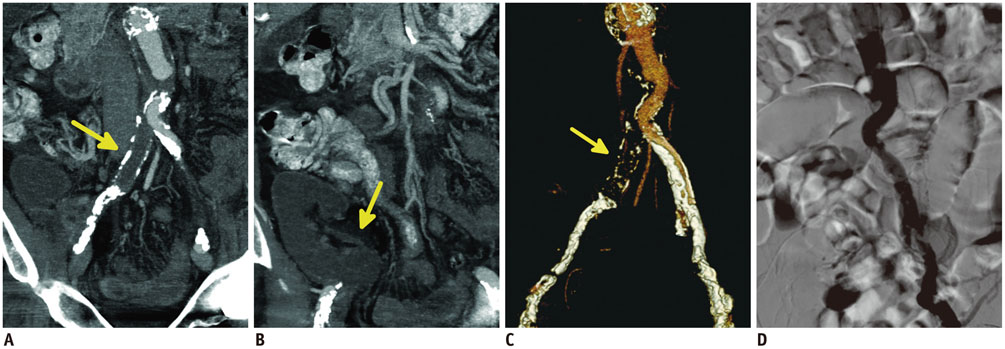
Fig. 8 70-year-old male is shown, who previously was surgically treated for large aortic aneurysm with aorto-iliac graft. A-D. Multiplanar reconstruction and volume-rendered reformatted images show thrombosis of right iliac branch, involving transplanted renal artery (arrows in A, C), without any enhancement of renal graft (arrow in B), as confirmed by digital subtraction angiography (D). Endovascular thrombolytic therapy was unsuccessful; graft was explanted 1 week later.
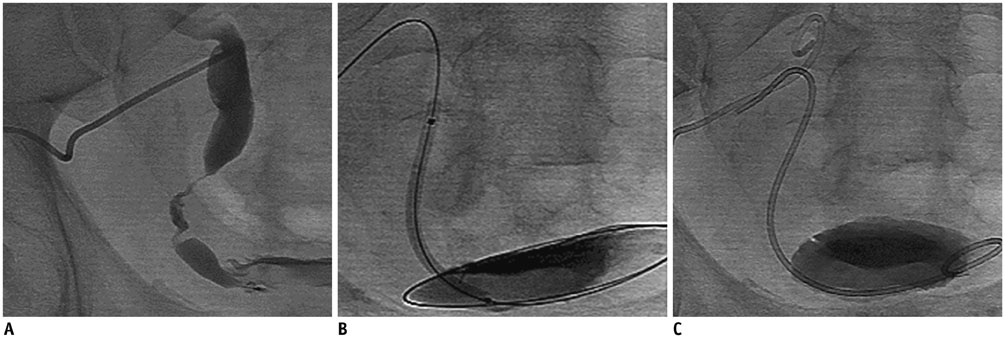
Fig. 9 60-year-old male is shown, presenting with increased creatinine levels and decreased urine output, 9 months after transplantation. A. Anterograde pyelogram shows distal ureteral stenosis with only minimal residual lumen. B, C. After accurate pre-dilatation of ureteral stenosis (percutaneous transluminal angioplasty-ballon: 5 × 40 mm, Wanda, Boston Scientific, USA) (B), double-J ureteral stent was successfully deployed (Flexima, Boston Scientific, USA) (C).

Fig. 10 Late-phase maximum intensity projection-thin CT-image shows uretero-neocystostomy.
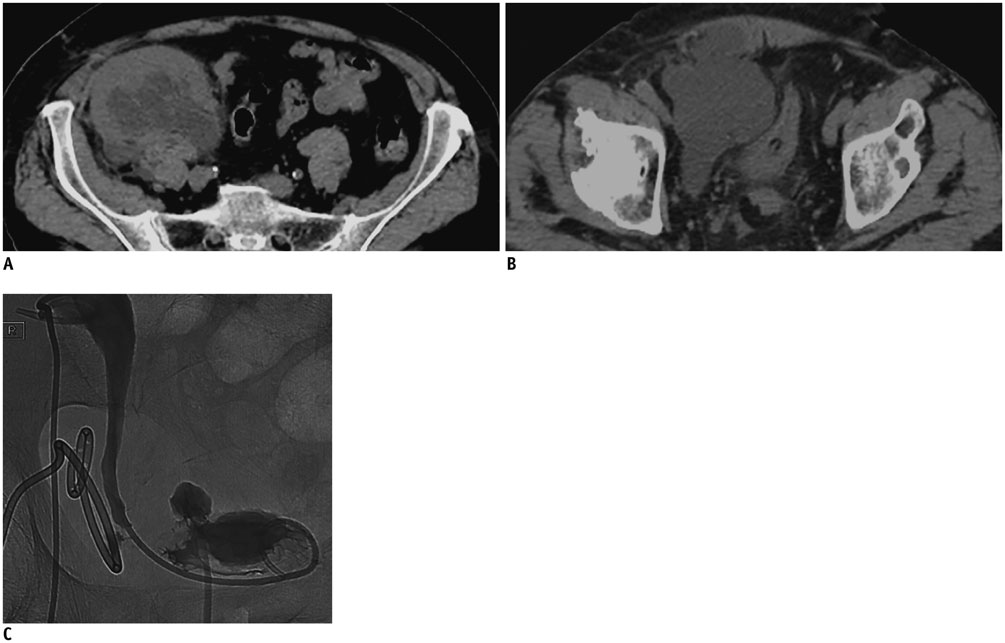
Fig. 11 49-year-old male is shown, who was complaining of pain and tenderness in right iliac fossa, 6 weeks after transplantation. A, B. Unenhanced CT scans show large, heterogeneous, multiloculated fluid collection. After successful positioning of 12-Fr drainage catheter, aspiration material analysis demonstrated urine content, confirming diagnosis of urinoma. C. Procedure was completed by double-J urinary stent deployment (Flexima, Boston Scientific, USA) with resolution of leak.

Fig. 12 65-year-old male is shown, at 25 days after transplantation. A, B. Late-phase MIP reconstructions demonstrate contrast-material leakage from uretero-neocystostomy anastomosis into large pelvic fluid collection (arrows). Aspiration material from 8-Fr drainage tube confirms diagnosis of urinoma. C. After deployment of 8-Fr nephrostomy, anterograde pyelogram demonstrates presence of urinary leakage into pelvic fluid collection. Failure to catheterize bladder prevented deployment of urinary stent, so patient was surgically treated by ureteral reimplantation. MIP = maximum intensity projection

Fig. 13 51-year-old female is shown, at 43 days after transplantation. A. Ultrasound (US) image shows large lymphocele, appearing as relatively anechoic multiloculated fluid collection compressing kidney. B. This complication was successfully treated by placing percutaneous drainage under US and fluoroscopic guidance.

Fig. 14 51-year-old male is shown, at 23 days after transplantation, presenting with fever, neutrophil leukocytosis, and purulent discharge from surgical incision. A. Ultrasound-image shows large perirenal fluid collection with hyperechoic content. B. 12-Fr double-lumen drainage cathether (vanSonnemberg, Boston Scientific, USA) was successfully deployed, with complete resolution of fluid collection in 4 days.
Reference
-
1. Wolfe RA, Ashby VB, Milford EL, Ojo AO, Ettenger RE, Agodoa LY, et al. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med. 1999; 341:1725–1730.2. Patel NH, Jindal RM, Wilkin T, Rose S, Johnson MS, Shah H, et al. Renal arterial stenosis in renal allografts: retrospective study of predisposing factors and outcome after percutaneous transluminal angioplasty. Radiology. 2001; 219:663–667.3. Matheus WE, Reis LO, Ferreira U, Mazzali M, Denardi F, Leitao VA, et al. Kidney transplant anastomosis: internal or external iliac artery? Urol J. 2009; 6:260–266.4. Rundback JH, Rizvi A, Tomasula J. Percutaneous treatment of transplant renal artery stenosis: techniques and results. Tech Vasc Interv Radiol. 1999; 2:91–97.5. Salvadori M, Di Maria L, Rosati A, Larti A, Piperno R, Becherelli P, et al. Efficacy and safety of Palmaz stent implantation in the treatment of renal artery stenosis in renal transplantation. Transplant Proc. 2005; 37:1047–1048.6. Peregrin JH, Bürgelová M. Restoration of failed renal graft function after successful angioplasty of pressure-resistant renal artery stenosis using a cutting balloon: a case report. Cardiovasc Intervent Radiol. 2009; 32:548–553.7. Hedegard W, Saad WE, Davies MG. Management of vascular and nonvascular complications after renal transplantation. Tech Vasc Interv Radiol. 2009; 12:240–262.8. Dimitroulis D, Bokos J, Zavos G, Nikiteas N, Karidis NP, Katsaronis P, et al. Vascular complications in renal transplantation: a single-center experience in 1367 renal transplantations and review of the literature. Transplant Proc. 2009; 41:1609–1614.9. Flechner SM, Novick AC. Renal transplantation. In : Gillenwater JY, Grayhack JT, Howards SS, Mitchell ME, editors. Adult and Pediatric Urology. 4th ed. Baltimore, MD: Lippincott Williams & Wilkins;2002. p. 941–954.10. Chen CH, Chen CH, Hsieh SR, Shu KH, Ho HC. Salvage of external iliac artery dissection immediately after renal transplant. Exp Clin Transplant. 2013; 11:274–277.11. Grenier N, Claudon M, Trillaud H, Douws C, Levantal O. Noninvasive radiology of vascular complications in renal transplantation. Eur Radiol. 1997; 7:385–391.12. Maleux G, Messiaen T, Stockx L, Vanrenterghem Y, Wilms G. Transcatheter embolization of biopsy-related vascular injuries in renal allografts. Long-term technical, clinical and biochemical results. Acta Radiol. 2003; 44:13–17.13. Ojo AO, Hanson JA, Wolfe RA, Agodoa LY, Leavey SF, Leichtman A, et al. Dialysis modality and the risk of allograft thrombosis in adult renal transplant recipients. Kidney Int. 1999; 55:1952–1960.14. Basić D, Hadzi-Djokić J, Milutinović D, Djokić M. [Vascular complications after kidney transplantation]. Srp Arh Celok Lek. 2003; 131:215–220.15. Rouvière O, Berger P, Béziat C, Garnier JL, Lefrançois N, Martin X, et al. Acute thrombosis of renal transplant artery: graft salvage by means of intra-arterial fibrinolysis. Transplantation. 2002; 73:403–409.16. Kaskarelis I, Koukoulaki M, Georgantas T, Bairamidis E, Kokkinos C, Ieronymou M, et al. Ureteral complications in renal transplant recipients successfully treated with interventional radiology. Transplant Proc. 2008; 40:3170–3172.17. Bhagat VJ, Gordon RL, Osorio RW, LaBerge JM, Kerlan RK Jr, Melzer JS, et al. Ureteral obstructions and leaks after renal transplantation: outcome of percutaneous antegrade ureteral stent placement in 44 patients. Radiology. 1998; 209:159–167.18. Yap R, Madrazo B, Oh HK, Dienst SG. Perirenal fluid collection after renal transplant. Am Surg. 1981; 47:287–290.19. Hariharan S, Johnson CP, Bresnahan BA, Taranto SE, McIntosh MJ, Stablein D. Improved graft survival after renal transplantation in the United States, 1988 to 1996. N Engl J Med. 2000; 342:605–612.20. Schwerk WB, Dürr HK. Ultrasound gray-scale pattern and guided aspiration puncture of abdominal abscesses. J Clin Ultrasound. 1981; 9:389–396.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Neurological Complications Following Liver Transplant: A Pictorial Review of Radiological and Clinical Findings
- The Utility of 64 Channel Multidetector CT Angiography for Evaluating the Renal Vascular Anatomy and Possible Variations: a Pictorial Essay
- Renal embolization for trauma: a narrative review
- The Role of Interventional Radiology in Treatment of Patients with Acute Trauma: A Pictorial Essay
- Clinical Findings and Interventional Treatment of Gastrointestinal Fistulae: Pictorial Essay
