Correlation of the Rotator Interval on Direct CT Arthrography in Shoulder Instability Patients with External Rotation Stress Radiographs
- Affiliations
-
- 1Department of Radiology, Hallym University College of Medicine, Dongtan Sacred Hospital, Hwaseong, Korea. jachoi88@gmail.com
- KMID: 2155277
- DOI: http://doi.org/10.3348/jksr.2016.74.3.177
Abstract
- PURPOSE
To correlate rotator interval dimensions on direct CT arthrography (CTA) with external rotation shoulder stress radiographs in patients with shoulder instability.
MATERIALS AND METHODS
One hundred and twenty-three shoulders of 115 patients with shoulder instability that underwent direct CTA and shoulder stress radiographs in neutral position and external rotation were enrolled. Axial, oblique coronal, oblique sagittal CT images were obtained after intra-articular contrast injection. Width and depth of rotator interval on sagittal CTA images were evaluated and acromiohumeral (AH) distance on neutral and external rotation stress radiographs were measured. CTA measurements were compared with AH on stress radiographs according to the group with or without "external rotational instability".
RESULTS
Out of 123 shoulders, 79 with external rotation instability showed increased or unchanged AH distance on external rotation compared with neutral position. Width of rotator interval was 2.43 +/- 0.31 cm and depth was 0.87 +/- 0.2 cm. Forty-four shoulders without external rotation instability showed decreased AH distance on external rotation compared with neutral position. Width of rotator interval was 2.02 +/- 0.45 cm and depth was 0.75 +/- 0.2 cm. Width and depth of rotator interval were significantly greater in the external rotation instability group.
CONCLUSION
Width and depth of rotator interval on CTA were significantly correlated with AH distance on external rotation stress radiographs.
Figure
-
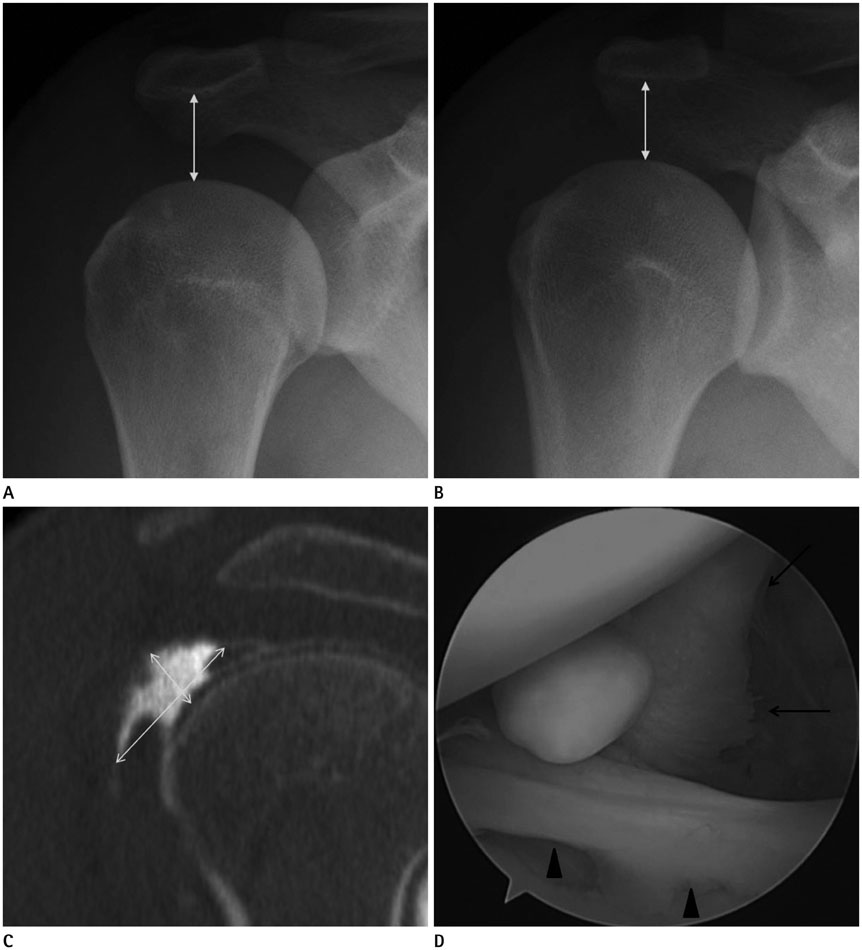
Fig. 1 A case of "external rotation instability positive". A. The stress radiograph in neutral position is obtained in a 27-year-old man with right shoulder instability. The acromiohumeral (AH) distance (double-headed arrow) is 1.93 cm. B. The AH distance on the stress radiograph in external rotation position (double-headed arrow) is 2.51 cm. There is increased AH distance compared to neutral stress radiograph. C. An oblique sagittal CT arthrographic image shows the rotator interval (RI) dimensions. The width of the RI (long arrow) is 2.29 cm and the depth (short arrow) is 0.88 cm. D. RI widening (arrows) is seen along with anteroinferior labral tear (arrowheads) at arthroscopy, so RI closure is performed.
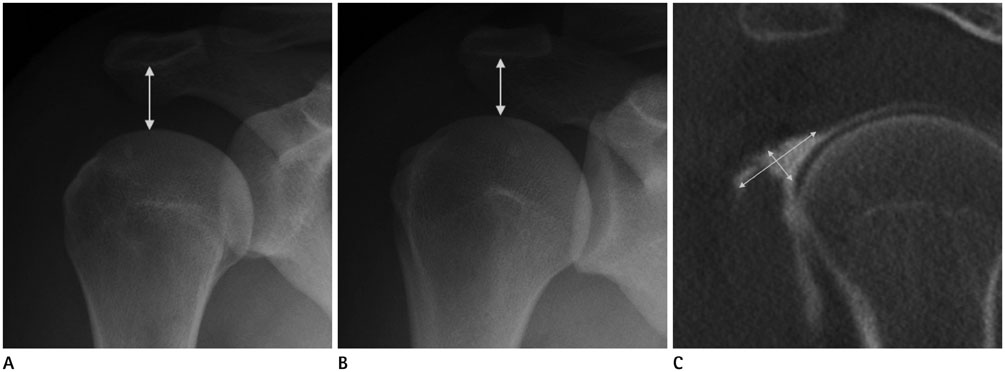
Fig. 2 A case of "external rotation instability negative". A. The stress radiograph in neutral position is obtained in 23-year-old man with right shoulder instability. The acromiohumeral (AH) distance (arrow) is 1.92 cm. B. The AH distance on the stress radiograph (arrow) in external rotation position is 1.66 cm. There is decreased AH distance compared to neutral stress radiograph. C. An oblique sagittal CT arthrographic image shows the rotator interval (RI) dimensions. The width of the RI (long arrow) is 1.88 cm and the depth (short arrow) is 0.54 cm.
Reference
-
1. Bigoni BJ, Chung CB. MR imaging of the rotator cuff interval. Radiol Clin North Am. 2006; 44:525–536. viii2. Krief OP. MRI of the rotator interval capsule. AJR Am J Roentgenol. 2005; 184:1490–1494.3. Itoi E, Berglund LJ, Grabowski JJ, Naggar L, Morrey BF, An KN. Superior-inferior stability of the shoulder: role of the coracohumeral ligament and the rotator interval capsule. Mayo Clin Proc. 1998; 73:508–515.4. Harryman DT 2nd, Sidles JA, Harris SL, Matsen FA 3rd. The role of the rotator interval capsule in passive motion and stability of the shoulder. J Bone Joint Surg Am. 1992; 74:53–66.5. Jost B, Koch PP, Gerber C. Anatomy and functional aspects of the rotator interval. J Shoulder Elbow Surg. 2000; 9:336–341.6. Pradhan RL, Itoi E. Rotator interval lesions of the shoulder joint. Orthopedics. 2001; 24:798–801. quiz 802-8037. Van der Reis W, Wolf EM. Arthroscopic rotator cuff interval capsular closure. Orthopedics. 2001; 24:657–661.8. Cole BJ, Mazzocca AD, Meneghini RM. Indirect arthroscopic rotator interval repair. Arthroscopy. 2003; 19:E28–E31.9. Field LD, Warren RF, O'Brien SJ, Altchek DW, Wickiewicz TL. Isolated closure of rotator interval defects for shoulder instability. Am J Sports Med. 1995; 23:557–563.10. Millett PJ, Clavert P, Warner JJ. Arthroscopic management of anterior, posterior, and multidirectional shoulder instability: pearls and pitfalls. Arthroscopy. 2003; 19:Suppl 1. 86–93.11. Cooper DE, O'Brien SJ, Arnoczky SP, Warren RF. The structure and function of the coracohumeral ligament: an anatomic and microscopic study. J Shoulder Elbow Surg. 1993; 2:70–77.12. Nobuhara K, Ikeda H. Rotator interval lesion. Clin Orthop Relat Res. 1987; (223):44–50.13. Fitzpatrick MJ, Powell SE, Tibone JE, Warren RF. The anatomy, pathology, and definitive treatment of rotator interval lesions: current concepts. Arthroscopy. 2003; 19:Suppl 1. 70–79.14. Nottage WM. Rotator interval lesions: physical exam, imaging, arthroscopic findings, and repair. Tech Shoulder Elbow Surg. 2003; 4:175–184.15. Chung CB, Dwek JR, Cho GJ, Lektrakul N, Trudell D, Resnick D. Rotator cuff interval: evaluation with MR imaging and MR arthrography of the shoulder in 32 cadavers. J Comput Assist Tomogr. 2000; 24:738–743.16. Ho CP. MR imaging of rotator interval, long biceps, and associated injuries in the overhead-throwing athlete. Magn Reson Imaging Clin N Am. 1999; 7:23–37.17. Wolf RS, Zheng N, Iero J, Weichel D. The effects of thermal capsulorrhaphy and rotator interval closure on multidirectional laxity in the glenohumeral joint: a cadaveric biomechanical study. Arthroscopy. 2004; 20:1044–1049.18. Gruber G, Bernhardt GA, Clar H, Zacherl M, Glehr M, Wurnig C. Measurement of the acromiohumeral interval on standardized anteroposterior radiographs: a prospective study of observer variability. J Shoulder Elbow Surg. 2010; 19:10–13.19. Gaskill TR, Braun S, Millett PJ. Multimedia article. The rotator interval: pathology and management. Arthroscopy. 2011; 27:556–556.20. Lee JC, Guy S, Connell D, Saifuddin A, Lambert S. MRI of the rotator interval of the shoulder. Clin Radiol. 2007; 62:416–423.21. Morag Y, Jacobson JA, Shields G, Rajani R, Jamadar DA, Miller B, et al. MR arthrography of rotator interval, long head of the biceps brachii, and biceps pulley of the shoulder. Radiology. 2005; 235:21–30.22. Beall DP, Morag Y, Ly JQ, Johnson MB, Pasque CB, Braley BA, et al. Magnetic resonance imaging of the rotator cuff interval. Semin Musculoskelet Radiol. 2006; 10:187–196.23. Vinson EN, Major NM, Higgins LD. Magnetic resonance imaging findings associated with surgically proven rotator interval lesions. Skeletal Radiol. 2007; 36:405–410.24. Taverna E, Sansone V, Battistella F. Arthroscopic rotator interval repair: the three-step all-inside technique. Arthroscopy. 2004; 20:Suppl 2. 105–109.25. Provencher MT, Dewing CB, Bell SJ, McCormick F, Solomon DJ, Rooney TB, et al. An analysis of the rotator interval in patients with anterior, posterior, and multidirectional shoulder instability. Arthroscopy. 2008; 24:921–929.26. Kim KC, Rhee KJ, Shin HD, Kim YM. Estimating the dimensions of the rotator interval with use of magnetic resonance arthrography. J Bone Joint Surg Am. 2007; 89:2450–2455.27. Lee HJ, Kim NR, Moon SG, Ko SM, Park JY. Multidirectional instability of the shoulder: rotator interval dimension and capsular laxity evaluation using MR arthrography. Skeletal Radiol. 2013; 42:231–238.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Assessment of anterior shoulder instability by CT arthrography
- Shoulder distention arthrography as a treatment modality
- Feasibility of Ultrasonography and MR Arthrography during Evaluation of Rotator Cuff Injury
- Ultrasonography and arthrography in rotator cuff lesions: algorithmic approach
- Comparison of Rotational Strength in Shoulders with Anterior Instability and Normal Shoulders Using Isokinetic Testing
