J Korean Ophthalmol Soc.
2015 Dec;56(12):1880-1886. 10.3341/jkos.2015.56.12.1880.
Vitrectomy with Perfluorocarbon Liquid versus Combined Encircling for Retinal Detachment with Giant Retinal Tear
- Affiliations
-
- 1Department of Ophthalmology, Pusan National University Yangsan Hospital, Yangsan, Korea. isbyon@naver.com
- 2Research Institute for Convergence of Biomedical Science and Technology, Pusan National University Yangsan Hospital, Yangsan, Korea.
- 3Department of Ophthalmology, Pusan National University Hospital, Busan, Korea.
- 4Department of Ophthalmology, Pusan National University School of Medicine, Busan, Korea.
- KMID: 2148749
- DOI: http://doi.org/10.3341/jkos.2015.56.12.1880
Abstract
- PURPOSE
To evaluate the clinical usefulness of additional encircling in patients treated for retinal detachment with giant retinal tear and without proliferative vitreoretinopathy, compared to single vitrectomy using perfluorocarbon liquid.
METHODS
Patients who underwent surgery for retinal detachment with giant retinal tear were divided into either the vitrectomy alone group or combined vitrectomy and encircling group. We reviewed the primary anatomical success rate, final anatomical success rate and best corrected visual acuity (BCVA) at the last follow-up (log MAR). Additionally, BCVA at the first visit, intraocular pressure, lens status, history of intraocular surgery, high myopia, trauma history, time from symptom onset to surgery, location and size of the giant retinal tear, extent of retinal detachment and foveal detachment were reviewed.
RESULTS
Among a total of 29 eyes, the vitrectomy alone group included 8 eyes and the combined group 21 eyes. Location and size of the giant retinal tear, extent of retinal detachment and foveal detachment, intraocular pressure, history of intraocular surgery, lens status, high myopia, trauma history and time from symptom onset to surgery were not different between the 2 groups. The primary success rate was 87.5% in the vitrectomy group and 85.7% in the combined group; the final surgery success rate was 100.0% and 95.2%, respectively. There was no significant difference in the anatomical success rate between the 2 groups. The postoperative BCVA was similar in both groups (0.80 vs. 0.92).
CONCLUSIONS
When vitrectomy using perfluorocarbon liquid was performed for the treatment of giant retinal tear without proliferative vitreoretinopathy, an encircling provided no additional benefit for the anatomical success rate and visual recovery. Only intensive vitrectomy of peripheral retina was considered capable of achieving a successful retinal attachment in patients without proliferative vitreoretinopathy.
MeSH Terms
Figure
-

Figure 1. Fundus photographs before and after retinal detachment repair. (A) Giant retinal tear is found from 2’30” to 6’ o’clock with retinal detachment with fovea off at baseline. (B) 6 months after removal of intraocular tamponade, retinal re-attachment is maintained.
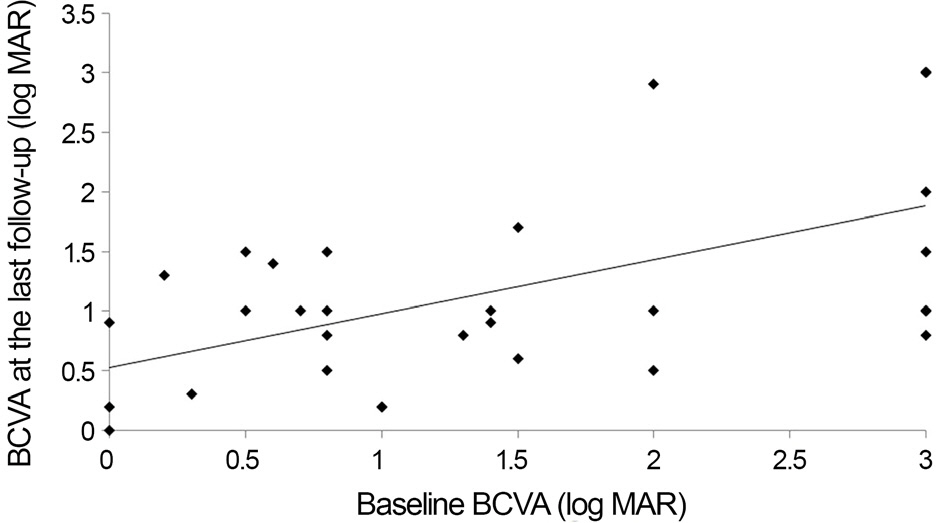
Figure 2. Correlations between best corrected visual acuity (BCVA) at the baseline and BCVA at the last follow-up. There is a significant correlation between baseline BCVA and post-operative BCVA at the last follow-up (r = 0.467, p = 0.001).
Reference
-
References
1. Dotrelova D, Karel I, Clupkova E. Retinal detachment in Marfan’s syndrome. Characteristics and surgical results. Retina. 1997; 17:390–6.2. Schepens CL, Dobble JG, McMeel JW. Retinal detachments with giant breaks: preliminary report. Trans Am Acad Ophthalmol Otolaryngol. 1962; 66:471–9.3. Monin C, Van Effenterre G, Andre-Sereys P, Haut J. Prevention of retinal detachment in Wagner-Stickler disease. Comparative study of different methods. Apropos of 22 cases. J Fr Ophtalmol. 1994; 17:167–74.4. Sarrazin L, Averbukh E, Halpert M. . Traumatic pediatric reti-nal detachment: a comparison between open and closed globe injuries. Am J Ophthalmol. 2004; 137:1042–9.
Article5. Machemer R, Allen AW. Retinal tears 180 degrees and greater. Management with vitrectomy and intravitreal gas. Arch Ophthalmol. 1976; 94:1340–6.6. Leaver PK, Lean JS. Management of giant retinal tears using vi-trectomy and silicone oil/fluid exchange. A preliminary report. Trans Ophthalmol Soc U K. 1981; 101:189–91.7. Faulborn J. Treatment of giant retinal tears after perforating in-juries with vitrectomy and a cyanocrylate tissue adhesive. Adv Ophthalmol. 1976; 33:204–7.8. Federman JL, Shakin JL, Lanning RC. The microsurgical manage-ment of giant retinal tears with trans-scleral retinal sutures. Ophthalmology. 1982; 89:832–9.
Article9. Ambresin A, Wolfensberger TJ, Bovey EH. Management of giant retinal tears with vitrectomy, internal tamponade, and peripheral 360 degrees retinal photocoagulation. Retina. 2003; 23:622–8.10. Ang GS, Townend J, Lois N. Epidemiology of giant retinal tears in the United Kingdom: the British Giant Retinal Tear Epidemiology Eye Study (BGEES). Invest Ophthalmol Vis Sci. 2010; 51:4781–7.
Article11. Kertes PJ, Wafapoor H, Peyman GA. . The management of giant retinal tears using perfluoroperhydrophenanthrene. A multi-center case series. Vitreon Collaborative Study Group. Ophthalmology. 1997; 104:1159–65.12. Gonzalez MA, Flynn HW Jr, Smiddy WE. . Giant retinal tears after prior pars plana vitrectomy: management strategies and outcomes. Clin Ophthalmol. 2013; 7:1687–91.
Article13. Thompson JA, Snead MP, Billington BM. . National audit of the outcome of primary surgery for rhegmatogenous retinal detachment. II. Clinical outcomes. Eye (Lond). 2002; 16:771–7.
Article14. Dabour SA. The outcome of surgical management for giant retinal tear more than 180°. BMC Ophthalmol. 2014; 14:86.
Article15. Kim WW, Kim JW, Kim JW. The clinical assessment of retinal de-tachment with giant retinal tear. J Korean Ophthalmol Soc. 2000; 41:2591–7.16. Aaberg TM Jr, Rubsamen PE, Flynn HW Jr. . Giant retinal tear as a complication of attempted removal of intravitreal lens frag-ments during cataract surgery. Am J Ophthalmol. 1997; 124:222–6.
Article17. Hernáez-Ortega MC, Soto-Pedre E. Bilateral retinal detachment associated with giant retinal tear following LASIK. J Refract Surg. 2003; 19:611.
Article18. Aylward GW, Cooling RJ, Leaver PK. Trauma-induced retinal de-tachment associated with giant retinal tears. Retina. 1993; 13:136–41.
Article19. Chou SC, Yang CH, Lee CH. . Characteristics of primary rheg-matogenous retinal detachment in Taiwan. Eye (Lond). 2007; 21:1056–61.
Article20. Malbran E, Dodds RA, Hulsbus R. . Retinal break type and proliferative vitreoretinopathy in nontraumatic retinal detachment. Graefes Arch Clin Exp Ophthalmol. 1990; 228:423–5.
Article21. Yorston DB, Wood ML, Gilbert C. Retinal detachment in East Africa. Ophthalmology. 2002; 109:2279–83.
Article22. Gonzalez MA, Flynn HW Jr, Smiddy WE. . Surgery for retinal detachment in patients with giant retinal tear: etiologies, manage-ment strategies, and outcomes. Ophthalmic Surg Lasers Imaging Retina. 2013; 44:232–7.
Article23. Ghosh YK, Banerjee S, Savant V. . Surgical treatment and out-come of patients with giant retinal tears. Eye (Lond). 2004; 18:996–1000.
Article24. Chang S, Lincoff H, Zimmerman NJ, Fuchs W. Giant retinal tears. Surgical techniques and results using perfluorocarbon liquids. Arch Ophthalmol. 1989; 107:761–6.25. Hoffman ME, Sorr EM. Management of giant retinal tears without scleral buckling. Retina. 1986; 6:197–204.
Article26. Kreiger AE, Lewis H. Management of giant retinal tears without scleral buckling. Use of radical dissection of the vitreous base and perfluoro-octane and intraocular tamponade. Ophthalmology. 1992; 99:491–7.27. Verstraeten T, Williams GA, Chang S. . Lens-sparing vi-trectomy with perfluorocarbon liquid for the primary treatment of giant retinal tears. Ophthalmology. 1995; 102:17–20.
Article28. Chang S. Perfluorocarbon liquids in vitreoretinal surgery. Int Ophthalmol Clin. 1992; 32:153–63.
Article29. Billington BM, Leaver PK. Vitrectomy and fluid/silicone-oil ex-change for giant retinal tears: results at 18 months. Graefes Arch Clin Exp Ophthalmol. 1986; 224:7–10.
Article30. Millsap CM, Peyman GA, Mehta NJ. . Perfluoroperhydro- phenanthrene (Vitreon) in the management of giant retinal tears: results of a collaborative study. Ophthalmic Surg. 1993; 24:759–63.31. Sirimaharaj M, Balachandran C, Chan WC. . Vitrectomy with short term postoperative tamponade using perfluorocarbon liquid for giant retinal tears. Br J Ophthalmol. 2005; 89:1176–9.
Article32. Unlü N, Kocaoğ lan H, Acar MA. . The management of giant retinal tears with silicone oil. Eur J Ophthalmol. 2003; 13:192–5.33. Al-Khairi AM, Al-Kahtani E, Kangave D, Abu El-Asrar AM. Prognostic factors associated with outcomes after giant retinal tear management using perfluorocarbon liquids. Eur J Ophthalmol. 2008; 18:270–7.
Article34. Goezinne F, LA Heij EC, Berendschot TT. . Low redetachment rate due to encircling scleral buckle in giant retinal tears treated with vitrectomy and silicone oil. Retina. 2008; 28:485–92.
Article35. Ie D, Glaser BM, Sjaarda RN. . The use of perfluoro-octane in the management of giant retinal tears without proliferative vitreoretinopathy. Retina. 1994; 14:323–8.
Article36. Bonnet M, Fleury J, Guenoun S. . Cryopexy in primary rheg-matogenous retinal detachment: a risk factor for postoperative pro-liferative vitreoretinopathy? Graefes Arch Clin Exp Ophthalmol. 1996; 234:739–43.37. Shunmugam M, Ang GS, Lois M. Giant retinal tears. Surv Ophthalmol. 2014; 59:192–216.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Perfluoro-N-octane as Postoperative Vitreous Substitutes in Retinal Detachment: A Case Report
- Clinical Evaluation of Perfluorocarbon Liquid in Retinal Detachment Surgery
- The Management of Giant Retinal Tear by use of Perfluorodecalin(DK-line(R) and Silicone Oil
- Scleral Encircling for Complex Types of Rhegmatogenous Retinal Detachment
- Surgical Results of the Uncomplicated Giant Retinal Breaks
