Clin Endosc.
2015 Sep;48(5):444-446. 10.5946/ce.2015.48.5.444.
Successful Removal of a Screw Nail in the Jejunum Using Double-Balloon Enteroscopy
- Affiliations
-
- 1Department of Internal Medicine, Sahmyook Medical Center, Seoul, Korea.
- 2Department of Internal Medicine, Seongbuk Joongang Hospital, Seoul, Korea.
- 3Institute for Digestive Research, Soonchunhyang University Hospital, Soonchunhyang University College of Medicine, Seoul, Korea. iman0825@schmc.ac.kr
- KMID: 2148559
- DOI: http://doi.org/10.5946/ce.2015.48.5.444
Abstract
- The vast majority of foreign bodies (FBs) that enter the stomach pass through the gastrointestinal tract spontaneously. When the FB enters the small bowel-beyond the reach of conventional endoscopy-daily radiographs are needed to ensure its safe passage. However, endoscopic intervention is an appropriate management strategy for a sharp-pointed FB, because sharp FBs have a higher risk of intestinal perforation. We describe here a case in which a 1.5-cm, sharp-pointed screw nail in the proximal jejunum was removed successfully by double-balloon enteroscopy from a 19-year-old-male with autism. This case adds to the growing body of evidence demonstrating the value of therapeutic double-balloon enteroscopy in the field of FB ingestion
Keyword
MeSH Terms
Figure
-
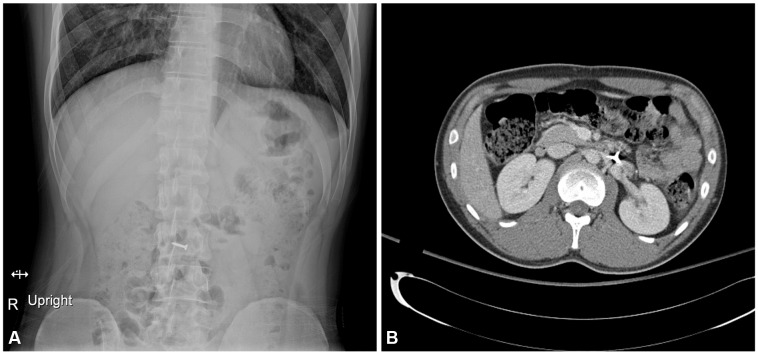
Fig. 1 Radiologic findings for an ingested sharp, pointed screw nail. (A) Abdominal simple radiography detected the presence of a sharp, pointed screw nail. (B) Abdominal computed tomography revealed a sharp, pointed screw nail in the proximal jejunum without evidence of small bowel perforation.
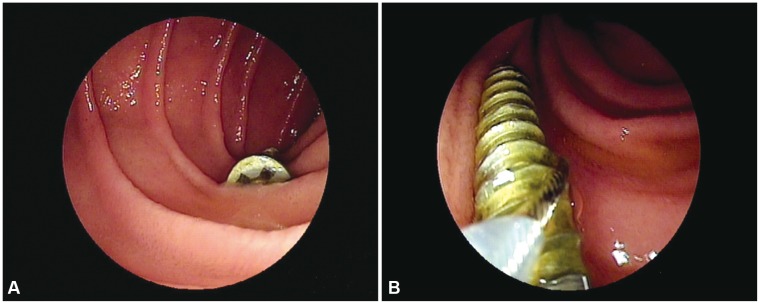
Fig. 2 Double-balloon enteroscopic findings of the ingested foreign body. (A) Double-balloon enteroscopy revealed a screw nail in the proximal jejunum without endoscopic evidence of perforation. (B) Endoscopic removal of the screw nail was attempted using a polypectomy snare. The screw nail in the jejunum was retrieved using a polypectomy snare.
Reference
-
1. Anderson KL, Dean AJ. Foreign bodies in the gastrointestinal tract and anorectal emergencies. Emerg Med Clin North Am. 2011; 29:369–400. ixPMID: 21515184.
Article2. Webb WA. Management of foreign bodies of the upper gastrointestinal tract: update. Gastrointest Endosc. 1995; 41:39–51. PMID: 7698623.
Article3. Rondonotti E, Sunada K, Yano T, Paggi S, Yamamoto H. Double-balloon endoscopy in clinical practice: where are we now? Dig Endosc. 2012; 24:209–219. PMID: 22725104.
Article4. Sugano K, Yamamoto H, Kita H. Double-Balloon Endoscopy: Theory and Practice. Tokyo: Springer;2006. p. 115.5. Kato S, Kani K, Takabayashi H, Yamamoto R, Yakabi K. Double balloon enteroscopy to retrieve an accidentally swallowed dental reamer deep in the jejunum. World J Gastrointest Endosc. 2011; 3:78–80. PMID: 21603036.
Article6. Shibuya T, Osada T, Asaoka D, et al. Double-balloon endoscopy for treatment of long-term abdominal discomfort due to small bowel penetration by an eel bone. Med Sci Monit. 2008; 14:CS107–CS109. PMID: 18830197.7. Tang SJ. Endoscopic management of foreign bodies in the gastrointestinal tract. Video J Encycl GI Endosc. 2013; 1:35–38.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Does Single Balloon Enteroscopy Have Similar Efficacy and Endoscopic Performance Compared with Double Balloon Enteroscopy?
- Diagnostic and Therapeutic Capability of Double-Balloon Enteroscopy in Clinical Practice
- A Case of a Cavernous Hemangioma in the Distal Jejunum Detected by Double-Balloon Enteroscopy in a Patient with Small Bowel Obstruction
- A Case of Inflammatory Myofibroblastic Tumor Diagnosed with Double-balloon Enteroscopy
- A Case of Bleeding from a Jejunal Gastrointestinal Stromal Tumor Diagnosed by Double Balloon Enteroscopy
