Cancer Res Treat.
2015 Jul;47(3):448-457. 10.4143/crt.2014.034.
Clinical Significance of Non-neutropenic Fever in the Management of Diffuse Large B-Cell Lymphoma Patients Treated with Rituximab-CHOP: Comparison with Febrile Neutropenia and Risk Factor Analysis
- Affiliations
-
- 1Division of Hematology-Oncology, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. kstwoh@skku.edu
- 2Division of Infectious Diseases, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2148494
- DOI: http://doi.org/10.4143/crt.2014.034
Abstract
- PURPOSE
Rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) is the standard chemotherapy in diffuse large B-cell lymphoma (DLBCL) patients. Although febrile neutropenia (FN) is the major toxicity of this regimen, non-neutropenic fever (NNF) becomes an emerging issue.
MATERIALS AND METHODS
We analyzed clinical features and outcomes of febrile complications from 397 patients with newly diagnosed DLBCL who were registered in the prospective cohort study. They had completed R-CHOP between September 2008 and January 2013.
RESULTS
Thirty-nine patients (9.8%) had NNF whereas 160 patients (40.3%) had FN. Among them, 24 patients (6.0%) had both during their treatment. Compared to frequent occurrence of initial FN after the first cycle (> 50% of total events), more than 80% of NNF cases occurred after the third cycle. Interstitial pneumonitis comprised the highest proportion of NNF cases (54.8%), although the causative organism was not identified in the majority of cases. Thus, pathogen was identified in a limited number of patients (n=9), and Pneumocystis jiroveci pneumonia (PJP) was the most common. Considering that interstitial pneumonitis without documented pathogen could be clinically diagnosed with PJP, the overall rate of PJP including probable cases was 4.5% (18 cases from 397 patients). The NNF-related mortality rate was 10.3% (four deaths from 39 patients with NNF) while the FN-related mortality rate was only 1.3%.
CONCLUSION
NNF was observed with incidence of 10% during R-CHOP treatment, and showed different clinical manifestations with respect to the time of initial episode and causes.
MeSH Terms
Figure
-
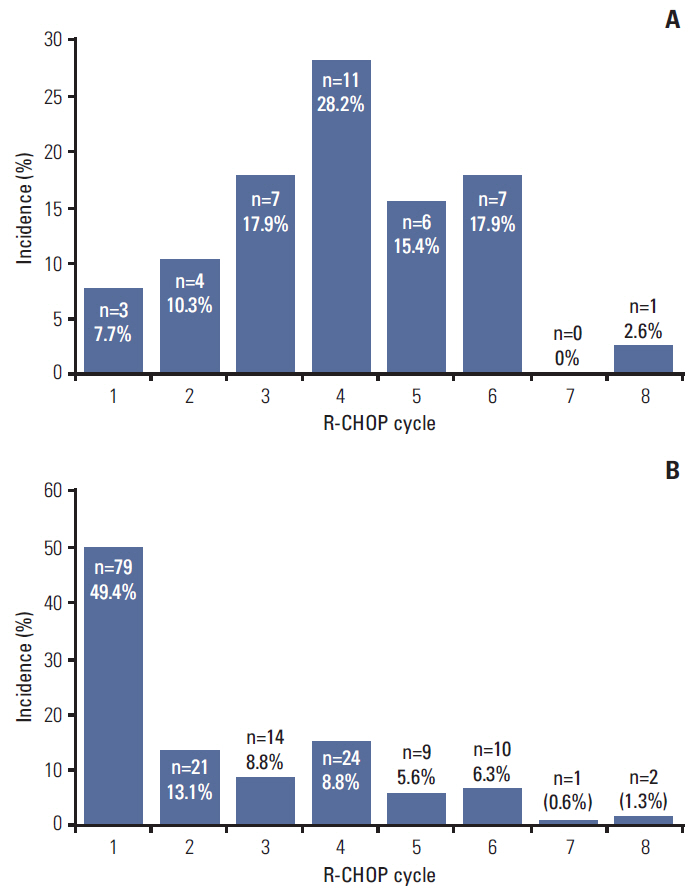
Fig. 1. Incidence of non-neutropenic fever (A) and febrile neutropenia (B) according to R-CHOP cycle. R-CHOP, rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone.
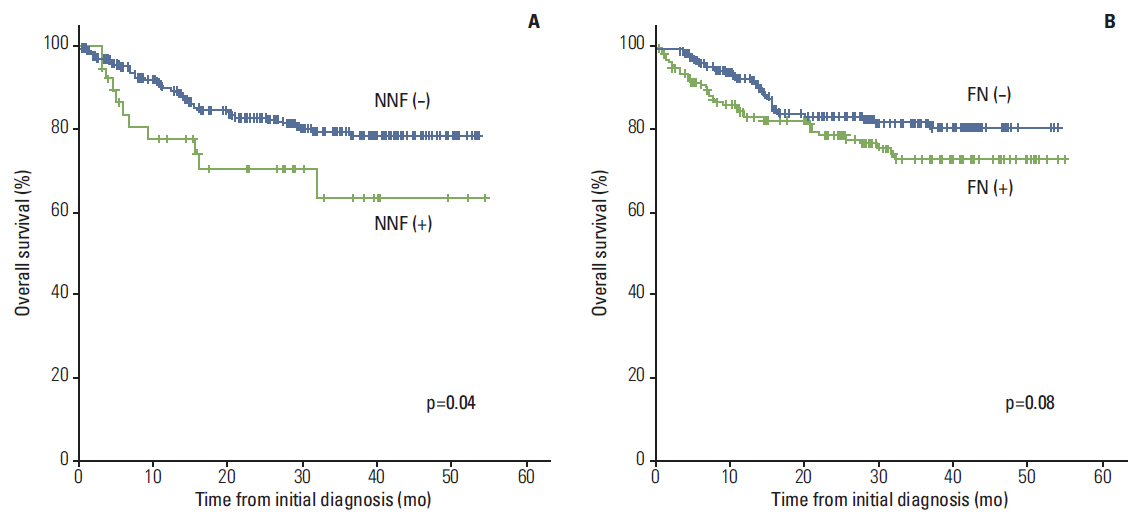
Fig. 2. Comparison of overall survival curves between patients with non-neutropenic fever (NNF) (A) or febrile neutropenia (FN) (B) and patients without any febrile event.
Reference
-
References
1. Huh J. Epidemiologic overview of malignant lymphoma. Korean J Hematol. 2012; 47:92–104.
Article2. Fisher RI, Gaynor ER, Dahlberg S, Oken MM, Grogan TM, Mize EM, et al. Comparison of a standard regimen (CHOP) with three intensive chemotherapy regimens for advanced non-Hodgkin's lymphoma. N Engl J Med. 1993; 328:1002–6.
Article3. Intragumtornchai T, Sutheesophon J, Sutcharitchan P, Swasdikul D. A predictive model for life-threatening neutropenia and febrile neutropenia after the first course of CHOP chemotherapy in patients with aggressive non-Hodgkin's lymphoma. Leuk Lymphoma. 2000; 37:351–60.
Article4. Klastersky J, Paesmans M, Rubenstein EB, Boyer M, Elting L, Feld R, et al. The Multinational Association for Supportive Care in Cancer risk index: a multinational scoring system for identifying low-risk febrile neutropenic cancer patients. J Clin Oncol. 2000; 18:3038–51.
Article5. de Souza Viana L, Serufo JC, da Costa Rocha MO, Costa RN, Duarte RC. Performance of a modified MASCC index score for identifying low-risk febrile neutropenic cancer patients. Support Care Cancer. 2008; 16:841–6.
Article6. Pettengell R, Bosly A, Szucs TD, Jackisch C, Leonard R, Paridaens R, et al. Multivariate analysis of febrile neutropenia occurrence in patients with non-Hodgkin lymphoma: data from the INC-EU Prospective Observational European Neutropenia Study. Br J Haematol. 2009; 144:677–85.
Article7. Pettengell R, Johnsen HE, Lugtenburg PJ, Silvestre AS, Duhrsen U, Rossi FG, et al. Impact of febrile neutropenia on R-CHOP chemotherapy delivery and hospitalizations among patients with diffuse large B-cell lymphoma. Support Care Cancer. 2012; 20:647–52.
Article8. Lanini S, Molloy AC, Fine PE, Prentice AG, Ippolito G, Kibbler CC. Risk of infection in patients with lymphoma receiving rituximab: systematic review and meta-analysis. BMC Med. 2011; 9:36.
Article9. Chen WL, Tsao YT, Chang TH, Chao TY, Kao WY, Chen YC, et al. Impact of interstitial pneumonia on the survival and risk factors analysis of patients with hematological malignancy. Biomed Res Int. 2013; 2013:185362.
Article10. Katsuya H, Suzumiya J, Sasaki H, Ishitsuka K, Shibata T, Takamatsu Y, et al. Addition of rituximab to cyclophosphamide, doxorubicin, vincristine, and prednisolone therapy has a high risk of developing interstitial pneumonia in patients with non-Hodgkin lymphoma. Leuk Lymphoma. 2009; 50:1818–23.
Article11. Kamel S, O'Connor S, Lee N, Filshie R, Nandurkar H, Tam CS. High incidence of Pneumocystis jirovecii pneumonia in patients receiving biweekly rituximab and cyclophosphamide, adriamycin, vincristine, and prednisone. Leuk Lymphoma. 2010; 51:797–801.12. Kolstad A, Holte H, Fossa A, Lauritzsen GF, Gaustad P, Torfoss D. Pneumocystis jirovecii pneumonia in B-cell lymphoma patients treated with the rituximab-CHOEP-14 regimen. Haematologica. 2007; 92:139–40.
Article13. Lyman GH, Delgado DJ. Risk and timing of hospitalization for febrile neutropenia in patients receiving CHOP, CHOP-R, or CNOP chemotherapy for intermediate-grade non-Hodgkin lymphoma. Cancer. 2003; 98:2402–9.
Article14. Lyman GH, Kuderer NM, Crawford J, Wolff DA, Culakova E, Poniewierski MS, et al. Predicting individual risk of neutropenic complications in patients receiving cancer chemotherapy. Cancer. 2011; 117:1917–27.
Article15. Kim T, Choi SH, Kim SH, Jeong JY, Woo JH, Kim YS, et al. Point prevalence of Pneumocystis pneumonia in patients with non-Hodgkin lymphoma according to the number of cycles of R-CHOP chemotherapy. Ann Hematol. 2013; 92:231–8.
Article16. Cooper N, Arnold DM. The effect of rituximab on humoral and cell mediated immunity and infection in the treatment of autoimmune diseases. Br J Haematol. 2010; 149:3–13.
Article17. Edwards JC, Cambridge G, Leandro MJ. B cell depletion therapy in rheumatic disease. Best Pract Res Clin Rheumatol. 2006; 20:915–28.
Article18. van der Kolk LE, Baars JW, Prins MH, van Oers MH. Rituximab treatment results in impaired secondary humoral immune responsiveness. Blood. 2002; 100:2257–9.
Article19. Stasi R, Cooper N, Del Poeta G, Stipa E, Laura Evangelista M, Abruzzese E, et al. Analysis of regulatory T-cell changes in patients with idiopathic thrombocytopenic purpura receiving B cell-depleting therapy with rituximab. Blood. 2008; 112:1147–50.
Article20. Bouaziz JD, Yanaba K, Venturi GM, Wang Y, Tisch RM, Poe JC, et al. Therapeutic B cell depletion impairs adaptive and autoreactive CD4+ T cell activation in mice. Proc Natl Acad Sci U S A. 2007; 104:20878–83.
Article21. Kurokawa T, Hase M, Tokuman N, Yoshida T. Immune reconstitution of B-cell lymphoma patients receiving CHOP-based chemotherapy containing rituximab. Hematol Oncol. 2011; 29:5–9.
Article22. Kaplan LD, Lee JY, Ambinder RF, Sparano JA, Cesarman E, Chadburn A, et al. Rituximab does not improve clinical outcome in a randomized phase 3 trial of CHOP with or without rituximab in patients with HIV-associated non-Hodgkin lymphoma: AIDS-Malignancies Consortium Trial 010. Blood. 2005; 106:1538–43.
Article23. Wagner SA, Mehta AC, Laber DA. Rituximab-induced interstitial lung disease. Am J Hematol. 2007; 82:916–9.
Article24. Ennishi D, Terui Y, Yokoyama M, Mishima Y, Takahashi S, Takeuchi K, et al. Increased incidence of interstitial pneumonia by CHOP combined with rituximab. Int J Hematol. 2008; 87:393–7.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Risk factors for neutropenic fever in non-Hodgkin’s lymphoma patients with primary granulocyte colony-stimulating factor prophylaxis
- Patterns of Neutropenia and Risk Factors for Febrile Neutropenia of Diffuse Large B-Cell Lymphoma Patients Treated with Rituximab-CHOP
- Additional rituximab-CHOP (R-CHOP) versus involved-field radiotherapy after a brief course of R-CHOP in limited, non-bulky diffuse large B-cell lymphoma: a retrospective analysis
- Risk Factors for Febrile Neutropenia during Chemotherapy for HIV-Related Lymphoma
- Prophylactic Effect of Pegfilgrastim on Febrile Neutropenia in Patients with Non-Hodgikin's Lymphoma
