Mitral-Aortic Intervalvular Fibrosa Pseudoaneurysm
- Affiliations
-
- 1Department of Cardiology, Laiko General Hospital, Athens, Greece. evapapadimitraki@hotmail.com
- 2First Department of Cardiology, Hippokration Hospital, University of Athens, Athens, Greece.
- 3Department of Cardiology, Athens Euroclinic, Athens, Greece.
- KMID: 2144457
- DOI: http://doi.org/10.4250/jcu.2015.23.4.257
Abstract
- Pseudoaneurysm of the mitral aortic intervalvular fibrosa (MAIVF-P) usually ensues as a complication of endocarditis or aortic valve surgery. When large, symptomatic or related to complications (rupture, compression of adjacent structures, embolic events, mitral regurgitation or heart failure) it warrants surgical excision. The natural course of uncomplicated/asymptomatic MAIVF-Ps is largely unknown since most patients are offered surgery. Increased surgical risk imposed by repeat operations in the majority of these patients is an important consideration and conservative treatment should not be excluded in selected cases. Herein we present two illustrative cases of MAIVF-P manifesting with significant arrhythmogenesis and complex endocarditis respectively. Both patients were managed conservatively. By briefly reviewing the existing literature, we discuss important diagnostic and therapeutic issues for MAIVF-Ps. To our knowledge complex ventricular arrhythmia has not been previously described as a prominent manifestation of MAIVF-P.
Keyword
MeSH Terms
Figure
-

Fig. 1 Significant arrhythmogenesis caused by a mitral-aortic intervalvular fibrosa pseudoaneurysm (MAIVF-P). A: 24-hour Holter recording of the patient in case 1. PVCs of multiple morphologies are depicted. The electrophysiologic study confirmed that the majority of those were of left ventricular outflow tract origin. B: Transesophageal echocardiogram (TEE), long axis view of the aorta systolic frame. A MAIVF-P exhibiting systolic expansion is seen (asterisk). C: TEE, long axis view of the aorta, color Doppler interrogation. The MAIVF-P fills during systole (arrow). AV: aortic valve, LA: left atrium, LV: left ventricle.

Fig. 2 Multidetector computed tomography showing the mitral-aortic intervalvular fibrosa pseudoaneurysm (arrows) both in the sagittal plane (A) and in the axial plane (B).
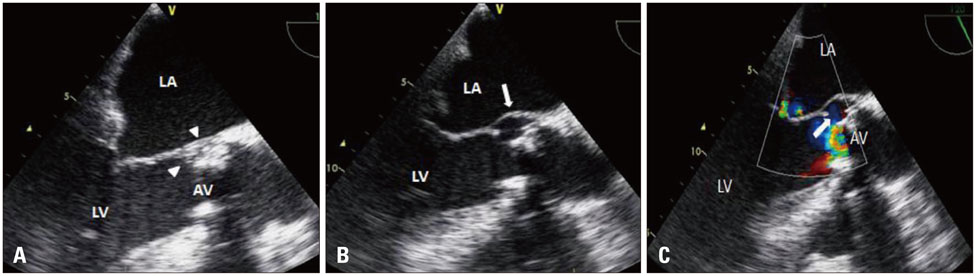
Fig. 3 The gradual formation of a pseidoaneurysm. A: Transesophageal echocardiogram (TEE), long axis view of the aorta. A small echodense space representing an abscess is seen in the mitral-aortic inetrvalvular fibrosa area (arrowheads). B: TEE, long axis view of the aorta, four weeks later. A mitral aortic intervalvular fibrosa pseudoaneurysm (MAIVF-P) at the site of the preexisting abscess is now depicted (arrow). C: TEE, long axis view of the aorta, color Doppler interrogation. The MAIVF-P communicates with the left ventricular outflow tract and fills during systole (arrow). AV: aortic valve, LV: left ventricle, LA: left atrium.
Reference
-
1. Redfearn DP, Hill JD, Keal R, Toff WD, Stafford PJ. Left ventricular dysfunction resulting from frequent unifocal ventricular ectopics with resolution following radiofrequency ablation. Europace. 2003; 5:247–250.2. Waldhausen JA, Petry EL, Kurlander GJ. Successful repair of subvalvular annular aneurysm of the left ventricle. N Engl J Med. 1966; 275:984–987.3. Sudhakar S, Sewani A, Agrawal M, Uretsky BF. Pseudoaneurysm of the mitral-aortic intervalvular fibrosa (MAIVF): a comprehensive review. J Am Soc Echocardiogr. 2010; 23:1009–1018. quiz 1112.4. Afridi I, Apostolidou MA, Saad RM, Zoghbi WA. Pseudoaneurysms of the mitral-aortic intervalvular fibrosa: dynamic characterization using transesophageal echocardiographic and Doppler techniques. J Am Coll Cardiol. 1995; 25:137–145.5. Tingleff J, Egeblad H, Gøtzsche CO, Baandrup U, Kristensen BO, Pilegaard H, Pettersson G. Perivalvular cavities in endocarditis: abscesses versus pseudoaneurysms? A transesophageal Doppler echocardiographic study in 118 patients with endocarditis. Am Heart J. 1995; 130:93–100.6. Daniel WG, Mügge A, Martin RP, Lindert O, Hausmann D, Nonnast-Daniel B, Laas J, Lichtlen PR. Improvement in the diagnosis of abscesses associated with endocarditis by transesophageal echocardiography. N Engl J Med. 1991; 324:795–800.7. Elhmidi Y, Günzinger R, Deutsch MA, Badiu CC, Krane M, Lange R. Outcomes of patients undergoing third-time aortic or mitral valve replacement. J Card Surg. 2014; 29:8–13.8. Hasin T, Reisner SA, Agmon Y. Large pseudoaneurysms of the mitralaortic intervalvular fibrosa: long-term natural history without surgery in two patients. Eur J Echocardiogr. 2011; 12:E24.9. Gin A, Hong H, Rosenblatt A, Black M, Ristow B, Popper R. Pseudoaneurysms of the mitral-aortic intervalvular fibrosa: survival without reoperation. Am Heart J. 2011; 161:130.e1–130.e5.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Mitral-aortic Intervalvular Fibrosa Pseudoaneurysm with Dual Fistula that Occurred in Prosthetic Aortic Valve Endocarditis
- Mitral-aortic Intervalvular Fibrosa Pseudoaneurysm with Dual Fistula and Complete AV Block after Aortic Valve Replacement in a Patients with Infective Endocarditis of Aortic Valve
- A Case of Mitral-Aortic Intervalvular Pseudoaneurysm with Fistula Complicating Native Aortic Valve Infective Endocarditis
- Anterior Mitral Leaflat Perforation in Patients with Bicuspid Aortic Valve Endocarditis
- Organizing Thrombus Mimicking a Cardiac Tumor Located at the Mitral-Aortic Intervalvular Fibrosa
