Accuracy of simulation surgery of Le Fort I osteotomy using optoelectronic tracking navigation system
- Affiliations
-
- 1Division of Dentistry, School of Dentistry, Seoul National University, Seoul, Korea. myungkim@snu.ac.kr
- 2Department of Oral & Maxillofacial Surgery, School of Dentistry, Seoul National University, Seoul, Korea.
- 3Dental Research Institute, Seoul National University, Seoul, Korea.
- KMID: 2137000
- DOI: http://doi.org/10.5125/jkaoms.2011.37.2.114
Abstract
- INTRODUCTION
The aim of this study was to demonstrate that the simulation surgery on rapid prototype (RP) model, which is based on the 3-dimensional computed tomography (3D CT) data taken before surgery, has the same accuracy as traditional orthograthic surgery with an intermediate splint, using an optoelectronic tracking navigation system.
MATERIALS AND METHODS
Simulation surgery with the same treatment plan as the Le Fort I osteotomy on the patient was done on a RP model based on the 3D CT data of 12 patients who had undergone a Le Fort I osteotomy in the department of oral and maxillofacial surgery, Seoul National University Dental Hospital. The 12 distances between 4 points on the skull, such as both infraorbital foramen and both supraorbital foramen, and 3 points on maxilla, such as the contact point of both maxillary central incisors and mesiobuccal cuspal tip of both maxillary first molars, were tracked using an optoelectronic tracking navigation system. The distances before surgery were compared to evaluate the accuracy of the RP model and the distance changes of 3D CT image after surgery were compared with those of the RP model after simulation surgery.
RESULTS
A paired t-test revealed a significant difference between the distances in the 3D CT image and RP model before surgery.(P<0.0001) On the other hand, Pearson's correlation coefficient, 0.995, revealed a significant positive correlation between the distances.(P<0.0001) There was a significant difference between the change in the distance of the 3D CT image and RP model in before and after surgery.(P<0.05) The Pearson's correlation coefficient was 0.13844, indicating positive correlation.(P<0.1)
CONCLUSION
Theses results suggest that the simulation surgery of a Le Fort I osteotomy using an optoelectronic tracking navigation system is relatively accurate in comparing the pre-, and post-operative 3D CT data. Furthermore, the application of an optoelectronic tracking navigation system may be a predictable and efficient method in Le Fort I orthognathic surgery.
Keyword
MeSH Terms
Figure
-
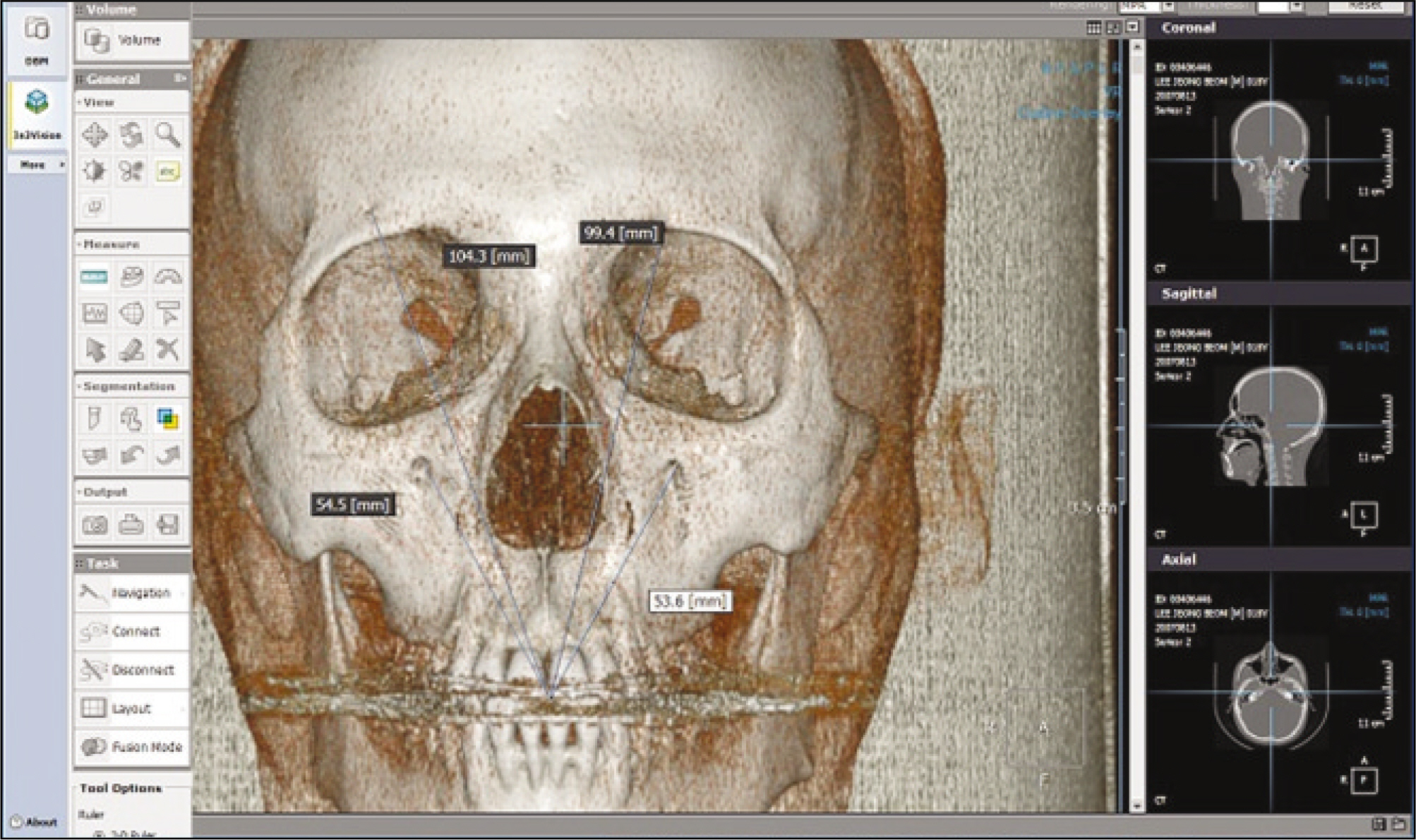
Fig. 1. Measuring the distance between 4 reference points and contact point of maxillary central incisors on a In2Vision 3-dimensional surgical navigation system.
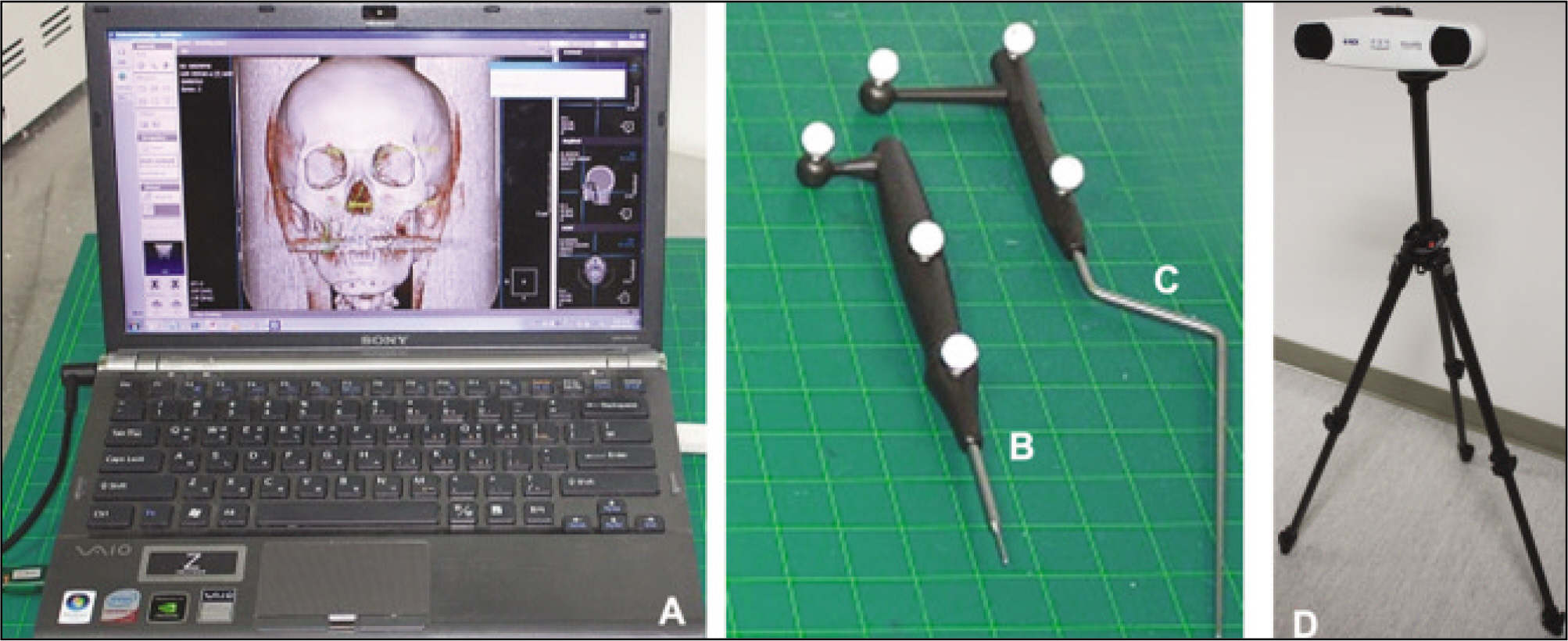
Fig. 2. Used tools in this study. A was the computer system displaying In2Vision system, B was the registration probe, C was the navigation probe, D was the infrared VICRA Polaris camera.

Fig. 3. Preparation and measurement of rapid prototype model in this study. A. Microscrews were implanted in nasion, both supraorbital foramen, contact point of maxillary central incisors for the reproducible measurement. B. Gradation was drawn over the maxillary canine and first molar and SAS was implanted in mesiobuccal cusp tip of maxillary first molar. C. Measuring the vertical distance between left supraorbital foramen and mesiobuccal cusp tip of left maxillary first molar. (SAS: skeletal anchoring system)

Fig. 4. Tracking the points by using of In2Vision 3 dimensional surgical navigation system and Polaris Vicra tracking device.
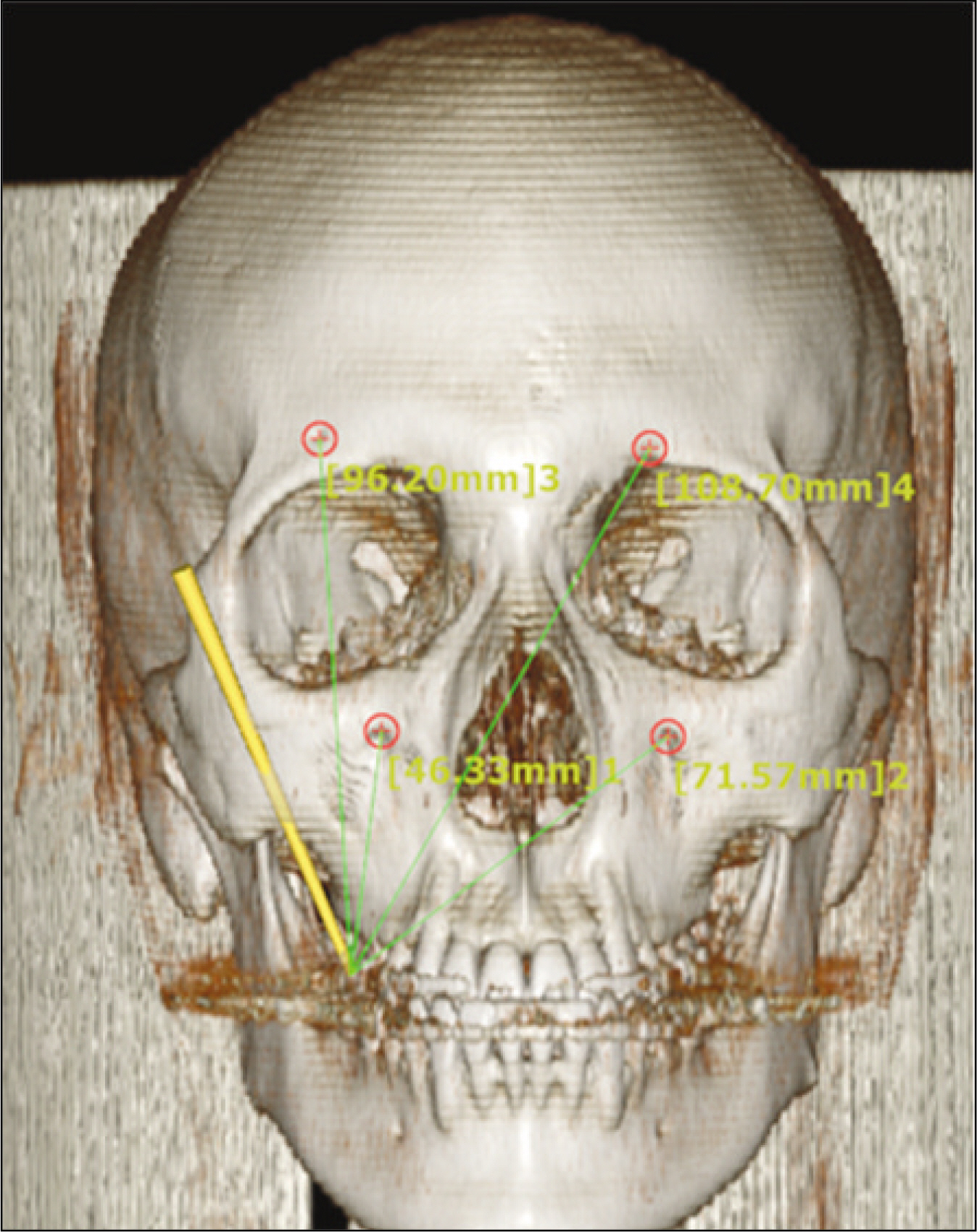
Fig. 5. Measuring the distance between 4 reference points on skull and ICP after simulation surgery on RP model (ICP: interincisal contact point, RP: rapid prototyping)

Fig. 6. RMSE analysis graph of measured distances between 3D CT image in X axis and RP model in Y axis before surgery.(mm) (RMSE: root mean square error, 3D CT: 3 dimensional computed tomography, RP: rapid prototyping)

Fig. 7. RMSE analysis graph showing changes between before and after surgery in measured distances of 3D CT image in X axis and RP model in Y axis.(mm) (RMSE: root mean square error, 3D CT: 3 dimensional computed tomography, RP: rapid prototyping)
Reference
-
References
1. Ewers R, Schicho K, Undt G, Wanschitz F, Truppe M, Seemann R, et al. Basic research and 12 years of clinical experience in computer-assisted navigation technology: a review. Int J Oral Maxillofac Surg. 2005; 34:1–8.
Article2. Klug C, Schicho K, Ploder O, Yerit K, Watzinger F, Ewers R, et al. Point-to-point computer-assisted navigation for precise transfer of planned zygoma osteotomies from the stereolithographic model into reality. J Oral Maxillofac Surg. 2006; 64:550–9.
Article3. Ellis E 3rd. Accuracy of model surgery: evaluation of an old technique and introduction of a new one. J Oral Maxillofac Surg. 1990; 48:1161–7.
Article4. Nizam A, Gopal RN, Naing L, Hakim AB, Samsudin AR. Dimensional Accuracy of the Skull Models Produced by Rapid Prototyping Technology Using Stereolithography Apparatus. Arch Orofac Sci. 2006; 1:60–6.5. Choi JY, Choi JH, Kim NK, Kim Y, Lee JK, Kim MK, et al. Analysis of errors in medical rapid prototyping models. Int J Oral Maxillofac Surg. 2002; 31:23–32.
Article6. Hassfeld S, Muhling J, Zoller J. Intraoperative navigation in oral and maxillofacial surgery. Int J Oral Maxillofac Surg. 1995; 24:111–9.7. Hassfeld S, Muhling J. Computer assisted oral and maxillofacial surgery-a review and an assessment of technology. Int J Oral Maxillofac Surg. 2001; 30:2–13.8. Wagner A, Ploder O, Enislidis G, Truppe M, Ewers R. Imageguided surgery, Int J Oral Maxillofac Surg. 1996; 25:147–51.9. Wagner A, Ploder O, Enislidis G, Truppe M, Ewers R. Virtual image guided navigation in tumor surgery-technical innovation, J Craniomaxillofac Surg. 1995; 23:271–3.10. Wagner A, Rasse M, Millesi W, et al. Virtual reality for orthognathic surgery: The augmented reality environment concept, J Oral Maxillofac Surg, 55, 456 (1997).11. Watzinger F, Birkfellner W, Wanschitz F, Ziya F, Wagner A, Kremser J, et al. Placement of endosteal implants in the zygoma after maxillectomy: a Cadaver study using surgical navigation. Plast Reconstr Surg. 2001; 107:659–67.
Article12. Ewers R, Schicho K, Wagner A, Undt G, Seemann R, Figl M, et al. Seven years of clinical experience with teleconsultation in craniomaxillofacial surgery. J Oral Maxillofac Surg. 2005; 63:1447–54.
Article13. Wagner A, Millesi W, Watzinger F, Truppe M, Rasse M, Enislidis G, et al. Clinical experience with interactive teleconsultation and teleassistance in craniomaxillofacial surgical procedures. J Oral Maxillofac Surg. 1999; 57:1413–8.
Article14. Eliashar R, Sichel JY, Gross M, Hocwald E, Dano I, Biron A, et al. Image of guided navigation system-a new technology for complex endoscopic endonasal surgery, Postgrad Med J. 2003; 79:686–90.15. Schicho K, Figl M, Seemann R, Ewers R, Lambrecht JT, Wagner A, et al. Accuracy of treatment planning based on stereolithography in computer assisted surgery. Med Phys. 2006; 33:3408–17.16. Jones RM, Khambay BS, McHugh S, Ayoub AF. The validity of a computer-assisted simulation system for orthognathic surgery (CASSOS) for planning the surgical correction of class III skeletal deformities: single-jaw versus bimaxillary surgery. Int J Oral Maxillofac Surg. 2007; 36:900–8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Le Fort I osteotomy as treatment for traumatic class III malocclusion caused by Le Fort III fracture: A case report
- A case report of surgical correction of mandibular prognathism with midfacial deficiency using Le Fort III osteotomy
- Two Cases of Epiphora Following Le Fort I Osteotomy
- Salvage rapid maxillary expansion for the relapse of maxillary transverse expansion after Le Fort I with parasagittal osteotomy
- Le Fort I Osteotomy and Posterior Maxillary Segmental Osteotomy for Correction of Malunioned Maxilla
