A Case of Right Ventricular Dysfunction Caused by Pectus Excavatum
- Affiliations
-
- 1Department of Cardiology, Dong-A University College of Medicine, Busan, Korea. thpark65@dau.ac.kr
- KMID: 2135441
- DOI: http://doi.org/10.4250/jcu.2010.18.2.62
Abstract
- Pectus excavatum compresses the underlying right side of the heart, which might lead to right ventricular dysfunction as illustrated in this case report.
Figure
-
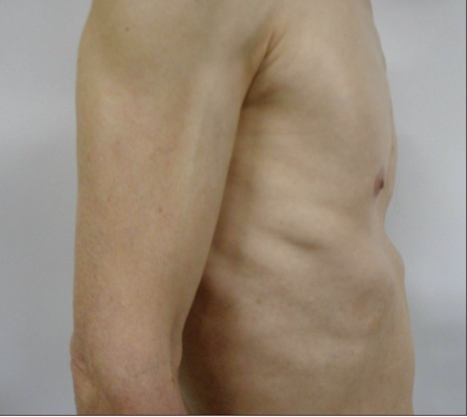
Fig. 1 On physical examination, depression of chest wall is apparent.

Fig. 2 Chest X-ray shows severe cardiomegaly, prominently of the right and left atria.
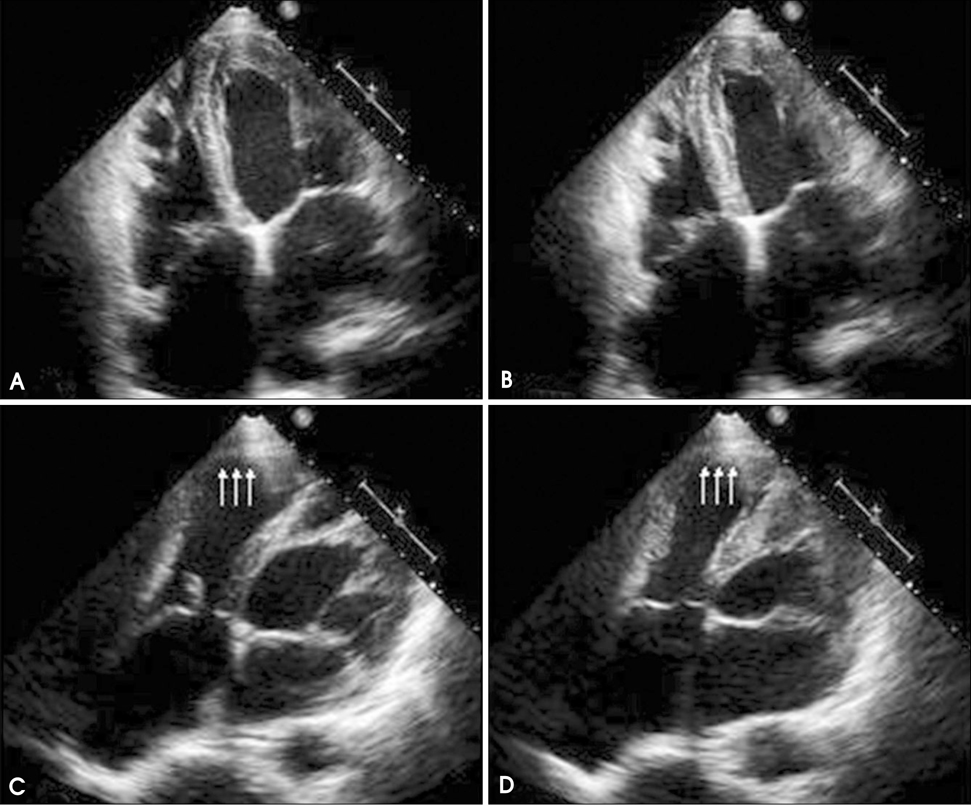
Fig. 3 Transthoracic echocardiography. Apical 4-chamber view in diastole (A) and systole (B) demonstrates reduced a fractional shortening area of right ventricular (RV). Modified 4-chamber view in diastole (C) and systole (D) shows an aneurysm-shaped RV apex which was akinetic (arrows).
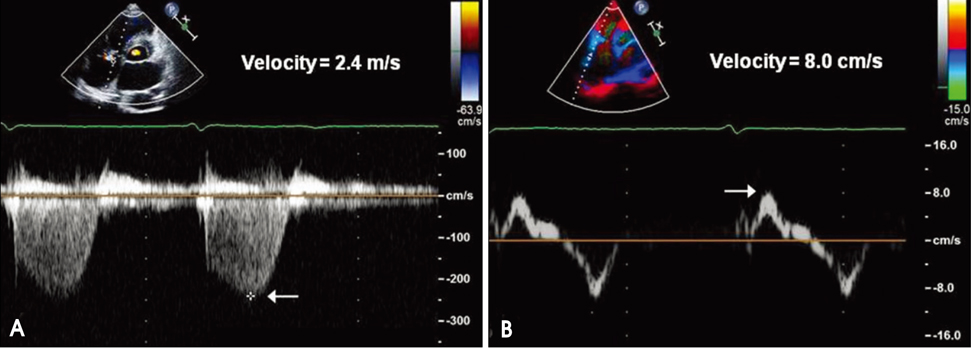
Fig. 4 The peak velocity of the tricuspid regurgitant jet is measured at 2.4 m/s (A) and tissue Doppler systolic velocity at the tricuspid annulus was 8.0 cm/s (B). Arrow indicates peak systolic velocity.
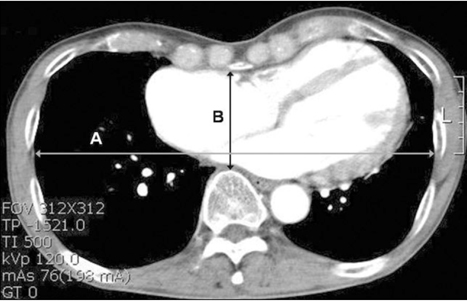
Fig. 5 Measurement of the Haller index. On chest computed tomography, Haller index is calculated by dividing the inner width of the chest at the widest point (A) by the distance between the posterior surface of the sternum and the anterior surface of the spine (B). Haller index of the patient is 4.2.
Reference
-
1. Fonkalsrud EW. Current management of pectus excavatum. World J Surg. 2003. 27:502–508.
Article2. Scherer LR, Arn PH, Dressel DA, Pyeritz RM, Haller JA Jr. Surgical management of children and young adults with Marfan syndrome and pectus excavatum. J Pediatr Surg. 1988. 23:1169–1172.
Article3. Wheeler R, Foote K. Pectus excavatum: studiously ignored in the United Kingdom? Arch Dis Child. 2000. 82:187–188.
Article4. Malek MH, Coburn JW. Strategies for cardiopulmonary exercise testing of pectus excavatum patients. Clinics (Sao Paulo). 2008. 63:245–254.
Article5. Raichura N, Entwisle J, Leverment J, Beardsmore CS. Breath-hold MRI in evaluating patients with pectus excavatum. Br J Radiol. 2001. 74:701–708.
Article6. Koumbourlis AC. Pectus excavatum: pathophysiology and clinical characteristics. Paediatr Respir Rev. 2009. 10:3–6.
Article7. Kelly RE Jr. Pectus excavatum: historical background, clinical picture, preoperative evaluation and criteria for operation. Semin Pediatr Surg. 2008. 17:181–193.
Article8. Mocchegiani R, Badano L, Lestuzzi C, Nicolosi GL, Zanuttini D. Relation of right ventricular morphology and function in pectus excavatum to the severity of the chest wall deformity. Am J Cardiol. 1995. 76:941–946.
Article9. Haller JA Jr, Kramer SS, Lietman SA. Use of CT scans in selection of patients for pectus excavatum surgery: a preliminary report. J Pediatr Surg. 1987. 22:904–906.
Article10. Haddad F, Doyle R, Murphy DJ, Hunt SA. Right ventricular function in cardiovascular disease, part II: pathophysiology, clinical importance, and management of right ventricular failure. Circulation. 2008. 117:1717–1731.
Article11. Shin MS. Right ventricle in echocardiography. J Korean Soc Echocardiogr. 2003. 11:76–80.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cardiac Cachexia Caused by Right Ventricular Outflow Tract Obstruction in a Patient With Severe Pectus Excavatum
- Repair of Recurrent Pectus Excavatum with a Huge Chest Wall Defect in a Patient with a Previous Ravitch and Pectus Bar Repair: A Case Report
- Simultaneous Nuss Operation and Mammoplasty in an Adult Patient with Pectus Excavatum: A case report
- Silastic Molding Method for Pectus Excavatum Correction Using a Polyvinyl Alcohol (Ivalon) Sponge
- Congenital Cystic Adenomatoid Malformation Associated with Pectus Excavatum: 1 case report
