Secondary Subaortic Stenosis after Patch Closure of Subarterial Ventricular Septal Defect
- Affiliations
-
- 1Department of Pediatrics, Chonnam National University Hospital, Chonnam National University Medical School, Gwangju, Korea. cardiol@jnu.ac.kr
- KMID: 2135438
- DOI: http://doi.org/10.4250/jcu.2010.18.2.52
Abstract
- Subaortic stenosis usually occurs without a previous heart operation, however, it can occur after heart surgery as well, with a condition known as a secondary subaortic stenosis (SSS). SSS has been reported after surgical repair of several congenital heart defects. There are only a few recorded cases of SSS after repair of ventricular septal defect (VSD). Here we report a rare case of SSS that occurred 3 years after surgical repair of subarterial VSD. A follow-up echocardiogram is essential for detecting SSS caused by the newly developed subaortic membrane in patients who had cardiac surgery.
MeSH Terms
Figure
-
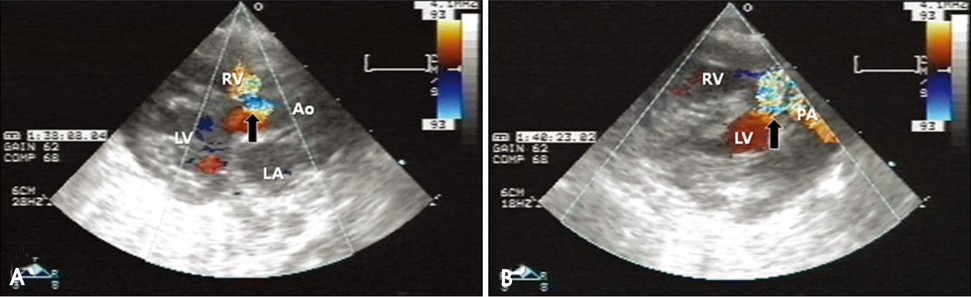
Fig. 1 Color Doppler imaging from parasternal long axis view (A) and parasternal short axis view (B) shows a large subarterial ventricular septal defect (arrows) at initial diagnosis. RV: right ventricle, LV: left ventricle, LA: left atrium, Ao: aorta, PA: pulmonary artery.

Fig. 2 After patch closure of the subartrial ventricular septal defect, echocardiography shows no discrete subaortic membrane (arrow) (A) and no blood flow disturbance in the left ventricular outflow tract (B). RV: right ventricle, LV: left ventricle, LA: left atrium, Ao: aorta.
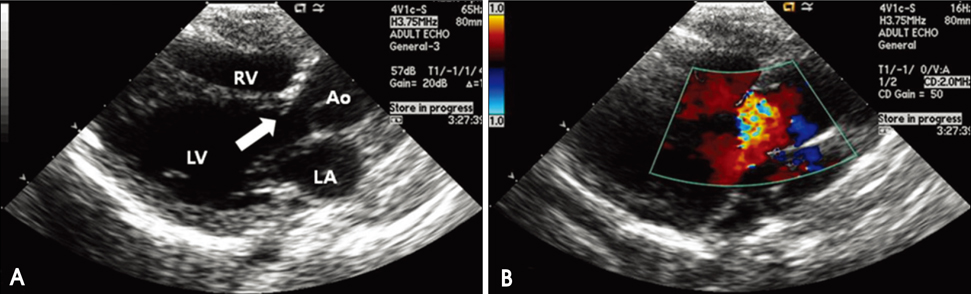
Fig. 3 Two dimensional echocardiography in the systolic phase shows subaortic stenosis (A) due to discrete subaortic membrane (arrow) and turbulent blood flow in the subaortic region during the systolic phase (B). RV: right ventricle, LV: left ventricle, LA: left atrium, Ao: aorta.
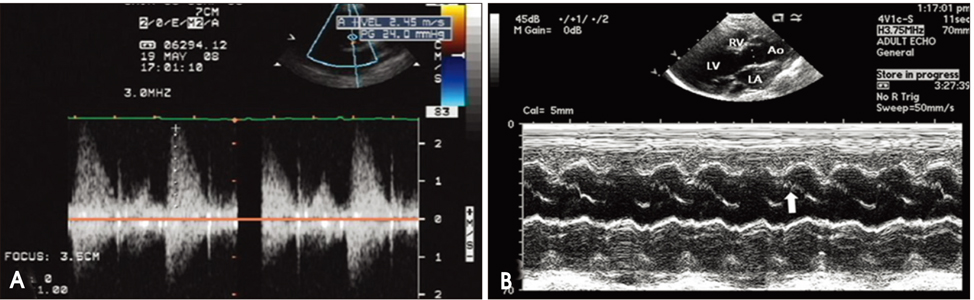
Fig. 4 Peak pressure gradient is estimated at 24 mmHg by Doppler echocardiography (A), and M-mode echocardiography shows a mid-systole partial closure of the aortic valve (arrow) (B). RV: right ventricle, LV: left ventricle, LA: left atrium, Ao: aorta.
Reference
-
1. Erentug V, Bozbuga N, Kirali K, Goksedef D, Akinci E, Isik O, Yakut C. Surgical treatment of subaortic obstruction in adolescent and adults: long-term follow-up. J Card Surg. 2005. 20:16–21.
Article2. Cho YS, Chang KS, Chin YK, Park KH, Youn SJ, Seo JC, Kim GY, Hong SP. Clinical observation on congenital heart disease in adult. J Korean Soc Echocardiogr. 1999. 7:23–31.
Article3. Kalfa D, Ghez O, Kreitmann B, Metras D. Secondary subaortic stenosis in heart defects without any initial subaortic obstruction: a multifactorial postoperative event. Eur J Cardiothorac Surg. 2007. 32:582–587.
Article4. Takeuchi K, McGowan FX Jr, Moran AM, Zurakowski D, Mayer JE Jr, Jonas RA, del Nido PJ. Surgical outcome of double-outlet right ventricle with subpulmonary VSD. Ann Thorac Surg. 2001. 71:49–52. discussion 52-3.
Article5. Cicini MP, Giannico S, Marino B, Iorio FS, Corno A, Marcelletti C. "Acquired" subvalvular aortic stenosis after repair of a ventricular septal defect. Chest. 1992. 101:115–118.
Article6. Razzouk AJ, Freedom RM, Cohen AJ, Williams WG, Trusler GA, Coles JG, Burrows PE, Rebeyka IM. The recognition, identification of morphologic substrate, and treatment of subaortic stenosis after a Fontan operation. An analysis of twelve patients. J Thorac Cardiovasc Surg. 1992. 104:938–944.
Article7. Serraf A, Zoghby J, Lacour-Gayet F, Houel R, Belli E, Galletti L, Planche C. Surgical treatment of subaortic stenosis: a seventeen-year experience. J Thorac Cardiovasc Surg. 1999. 117:669–678.
Article8. Gurbuz AT, Novick WM, Pierce CA, Watson DC. Left ventricular outflow tract obstruction after partial atrioventricular septal defect repair. Ann Thorac Surg. 1999. 68:1723–1726.
Article9. Lampros TD, Cobanoglu A. Discrete subaortic stenosis: an acquired heart disease. Eur J Cardiothorac Surg. 1998. 14:296–303.
Article10. Brauner R, Laks H, Drinkwater DC Jr, Shvarts O, Eghbali K, Galindo A. Benefits of early surgical repair in fixed subaortic stenosis. J Am Coll Cardiol. 1997. 30:1835–1842.
Article11. Kleinert S, Geva T. Echocardiographic morphometry and geometry of the left ventricular outflow tract in fixed subaortic stenosis. J Am Coll Cardiol. 1993. 22:1501–1508.
Article12. van Son JA, Schaff HV, Danielson GK, Hagler DJ, Puga FJ. Surgical treatment of discrete and tunnel subaortic stenosis. Late survival and risk of reoperation. Circulation. 1993. 88:II159–II169.13. Cohen L, Bennani R, Hulin S, Malergue MC, Yemets I, Kalangos A, Murrith N, Ouaknine R, Lecompte Y. Mitral valvar anomalies and discrete subaortic stenosis. Cardiol Young. 2002. 12:138–146.
Article14. Van Praagh R, Corwin RD, Dahlquist EH Jr, Freedom RM, Mattioli L, Nebesar RA. Tetralogy of Fallot with severe left ventricular anomalous attachment of the mitral valve to the ventricular septum. Am J Cardiol. 1970. 26:93–101.
Article15. Gersony WM. Natural history of discrete subvalvar aortic stenosis: management implications. J Am Coll Cardiol. 2001. 38:843–845.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Echocardiographic Study of the Ventricular Septal Defect with Subaortic Ridge
- A case of discrete subaortic stenosis
- Cinical Study of Spontaneous Closure in Simple Ventricular Septal Defects
- Subaortic stenosis: Anatomic Patterns and Associated Cardiovascular Abnormalities
- A Case of Traumatic Ventricular Septal Defect Secondary to Nonpenetrating Chest Trauma
