Comparison of Myocardial Contrast Echocardiography Versus Rest Sestamibi Myocardial Perfusion Imaging in the Early Diagnosis of Acute Coronary Syndrome
- Affiliations
-
- 1Division of Cardiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. dhkang@amc.seoul.kr
- KMID: 2135437
- DOI: http://doi.org/10.4250/jcu.2010.18.2.45
Abstract
- BACKGROUND
It remains unclear whether myocardial contrast echocardiography (MCE) is as accurate as myocardial perfusion imaging with technetium-99m sestamibi (MPI) for the diagnosis of acute coronary syndrome (ACS). We sought to directly compare the diagnostic accuracy of MCE with resting MPI in a head-to-head fashion.
METHODS
We prospectively enrolled 98 consecutive patients (mean age; 59+/-9 years, 68 males) who presented to the emergency department with chest pain suggestive of acute myocardial ischemia. Early MCE was performed by using continuous infusion of perfluorocarbon-exposed sonicated dextrose albumin (PESDA) during intermittent power Doppler harmonic imaging. Myocardial perfusion defects observed in at least one coronary territory were considered positive. Sestamibi was injected immediately after MCE and MPI was obtained within 6 hours of tracer injection.
RESULTS
ACS was confirmed in 67 patients. There were 32 patients with acute myocardial infarction (AMI) and 35 patients with unstable angina requiring urgent revascularization. The sensitivities of MCE and MPI for the diagnosis of ACS were 72% and 61%, respectively, which were significantly higher than those of ST segment change (24%, p<0.001 vs. MCE and vs. MPI) and troponin I (27%, p<0.001 vs. MCE and vs. MPI), with similar specificities of 90% to 100%. On a receiveroperating characteristics curve demonstrating diagnostic accuracy for ACS, the area under the curve of MCE was significantly larger than that of MPI (0.86 vs. 0.77, respectively; p=0.019).
CONCLUSION
MCE and MPI overcome the low sensitivity of routine triage tests for detecting ACS, and MCE is more accurate than MPI for the diagnosis of ACS in the emergency department.
MeSH Terms
Figure
-
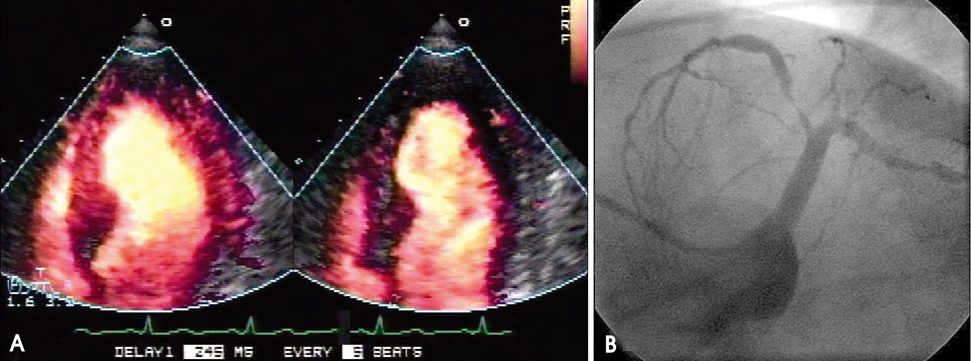
Fig. 1 Myocardial contrast echocardiography using power harmonic Doppler imaging with a dual-frame triggering (A). Left, perfusion frame was generated when the first packet of pulses encountered microbubbles in the myocardium and destroyed them. Right, post-destruction frame was obtained approximately 50 milliseconds later demonstrating the myocardium which was void of microbubbles. Apical perfusion defects are observed in the first perfusion imaging frame with 1 : 5 trigger rate. There was moderately decreased perfusion of the left anterior descending artery territory on myocardial perfusion imaging and critical stenosis of the left anterior descending artery on coronary angiography (B).
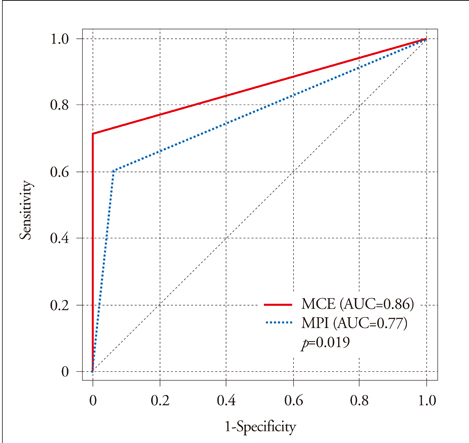
Fig. 2 Receiver-operating characteristics curve comparing the accuracy of myocardial contrast echocardiography (MCE) and myocardial perfusion imaging (MPI) for diagnosis of acute coronary syndrome (ACS). The area under the curve (AUC) of MCE was significantly larger than that of MPI (0.86 and 0.77, p=0.019).
Reference
-
1. Selker HP, Zalenski RJ, Antman EM, Aufderheide TP, Bernard SA, Bonow RO, Gibler WB, Hagen MD, Johnson P, Lau J, McNutt RA, Ornato J, Schwartz JS, Scott JD, Tunick PA, Weaver WD. An evaluation of technologies for identifying acute cardiac ischemia in the emergency department: a report from a National Heart Attack Alert Program Working Group. Ann Emerg Med. 1997. 29:13–87.
Article2. Pope JH, Ruthazer R, Beshansky JR, Griffith JL, Selker HP. Clinical Features of Emergency Department Patients Presenting with Symptoms Suggestive of Acute Cardiac Ischemia: A Multicenter Study. J Thromb Thrombolysis. 1998. 6:63–74.3. Fineberg HV, Scadden D, Goldman L. Care of patients with a low probability of acute myocardial infarction. Cost-effectiveness of alternatives to coronary-care-unit admission. N Engl J Med. 1984. 310:1301–1307.
Article4. Beller GA. Beller GA, editor. Radiopharmaceuticals in nuclear cardiology. Clinical Nuclear Cardiology. 1995. Philadelphia, PA: Saunders;37–81.5. Kontos MC, Jesse RL, Schmidt KL, Ornato JP, Tatum JL. Value of acute rest sestamibi perfusion imaging for evaluation of patients admitted to the emergency department with chest pain. J Am Coll Cardiol. 1997. 30:976–982.
Article6. Udelson JE, Beshansky JR, Ballin DS, Feldman JA, Griffith JL, Handler J, Heller GV, Hendel RC, Pope JH, Ruthazer R, Spiegler EJ, Woolard RH, Selker HP. Myocardial perfusion imaging for evaluation and triage of patients with suspected acute cardiac ischemia: a randomized controlled trial. JAMA. 2002. 288:2693–2700.
Article7. Jeetley P, Burden L, Greaves K, Senior R. Prognostic value of myocardial contrast echocardiography in patients presenting to hospital with acute chest pain and negative troponin. Am J Cardiol. 2007. 99:1369–1373.
Article8. Kaul S, Senior R, Dittrich H, Raval U, Khattar R, Lahiri A. Detection of coronary artery disease with myocardial contrast echocardiography: comparison with 99mTc-sestamibi single-photon emission computed tomography. Circulation. 1997. 96:785–792.
Article9. Jeetley P, Hickman M, Kamp O, Lang RM, Thomas JD, Vannan MA, Vanoverschelde JL, van der Wouw PA, Senior R. Myocardial contrast echocardiography for the detection of coronary artery stenosis: a prospective multicenter study in comparison with single-photon emission computed tomography. J Am Coll Cardiol. 2006. 47:141–145.
Article10. Senior R, Lepper W, Pasquet A, Chung G, Hoffman R, Vanoverschelde JL, Cerqueira M, Kaul S. Myocardial perfusion assessment in patients with medium probability of coronary artery disease and no prior myocardial infarction: comparison of myocardial contrast echocardiography with 99mTc single-photon emission computed tomography. Am Heart J. 2004. 147:1100–1105.
Article11. Lee CW, Moon DH, Hong MK, Lee JH, Choi SW, Yang HS, Kim JJ, Park SW, Park SJ. Effect of abciximab on myocardial salvage in patients with acute myocardial infarction undergoing primary angioplasty. Am J Cardiol. 2002. 90:1243–1246.
Article12. Kontos MC, Jesse RL, Anderson FP, Schmidt KL, Ornato JP, Tatum JL. Comparison of myocardial perfusion imaging and cardiac troponin I in patients admitted to the emergency department with chest pain. Circulation. 1999. 99:2073–2078.
Article13. Ohman EM, Armstrong PW, Christenson RH, Granger CB, Katus HA, Hamm CW, O'Hanesian MA, Wagner GS, Kleiman NS, Harrell FE Jr, Califf RM. GUSTO IIA Investigators. Cardiac troponin T levels for risk stratification in acute myocardial ischemia. N Engl J Med. 1996. 335:1333–1341.
Article14. Porter TR, Xie F. Visually discernible myocardial echocardiographic contrast after intravenous injection of sonicated dextrose albumin microbubbles containing high molecular weight, less soluble gases. J Am Coll Cardiol. 1995. 25:509–515.
Article15. Heinle SK, Noblin J, Goree-Best P, Mello A, Ravad G, Mull S, Mammen P, Grayburn PA. Assessment of myocardial perfusion by harmonic power Doppler imaging at rest and during adenosine stress: comparison with (99m)Tc-sestamibi SPECT imaging. Circulation. 2000. 102:55–60.
Article16. Kang DH, Kang SJ, Song JM, Choi KJ, Hong MK, Song JK, Park SW, Park SJ. Efficacy of myocardial contrast echocardiography in the diagnosis and risk stratification of acute coronary syndrome. Am J Cardiol. 2005. 96:1498–1502.
Article17. DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988. 44:837–845.
Article18. Hilton TC, Thompson RC, Williams HJ, Saylors R, Fulmer H, Stowers SA. Technetium-99m sestamibi myocardial perfusion imaging in the emergency room evaluation of chest pain. J Am Coll Cardiol. 1994. 23:1016–1022.
Article19. Rinkevich D, Kaul S, Wang XQ, Tong KL, Belcik T, Kalvaitis S, Lepper W, Dent JM, Wei K. Regional left ventricular perfusion and function in patients presenting to the emergency department with chest pain and no ST-segment elevation. Eur Heart J. 2005. 26:1606–1611.
Article20. Kaul S, Senior R, Firschke C, Wang XQ, Lindner J, Villanueva FS, Firozan S, Kontos MC, Taylor A, Nixon IJ, Watson DD, Harrell FE. Incremental value of cardiac imaging in patients presenting to the emergency department with chest pain and without ST-segment elevation: a multicenter study. Am Heart J. 2004. 148:129–136.
Article21. DePuey EG, Rozanski A. Using gated technetium-99m-sestamibi SPECT to characterize fixed myocardial defects as infarct or artifact. J Nucl Med. 1995. 36:952–955.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Correlation between Reverse Redistribution and Subendocardial Myocardial Infarction Observed in Myocardial Contrast Echocardiography
- Stress Testing and Imaging Protocols for Myocardial Perfusion Studies
- Nuclear Cardiology in Acute Coronary Syndrome
- Assessments of myocardial perfusion in human using stress intravenous PESDA myocardial contrast echocardiography and Pulse Inversion Harmonic Imaging: A Comparison study with Tc-99m sestamibi SPECT
- Assessment of collateral flow and myocardial perfusion by myocardial contrast echocardiography after coronary vasodiator during acute coronary occlusion
