A Typical Case of L-Transposition of the Great Arteries Initially Presented as Complete Atrioventricular Block in Middle-Aged Man
- Affiliations
-
- 1Cardiovascular Center, Korea University Guro Hospital, Seoul, Korea. jinona@medimail.co.kr
- KMID: 2135405
- DOI: http://doi.org/10.4250/jcu.2015.23.1.36
Abstract
- L-transposition of the great arteries (L-TGA) is a rare congenital anomaly and could cause complete atrioventricular (AV) block at relatively younger age. We present a case of 43-year-old male who complained of dizziness due to complete AV block. We confirmed L-TGA using transthoracic echocardiography and cardiac computed tomography. Permanent pacemaker was inserted without complications. No invasive treatment including corrective surgery was performed because patient's cardiac function was almost normal and the symptom was completely resolved after pacemaker insertion.
MeSH Terms
Figure
-
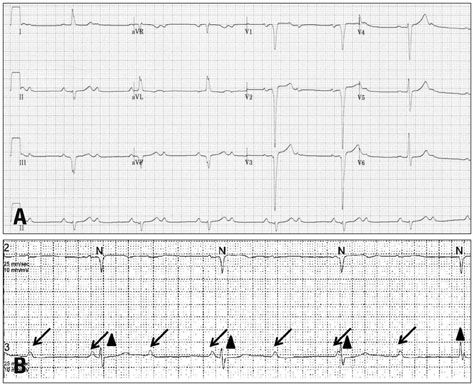
Fig. 1 Electrocardiogram (A) and Holter (B) on admission. 2:1 atrioventricular (AV) block, Q wave in right precordial limb lead (V1, II, III), absent Q wave in left precordial lead (V5, V6) and left axis deviation (A), complete AV block (B) (arrow: P wave, arrowhead: QRS complex).
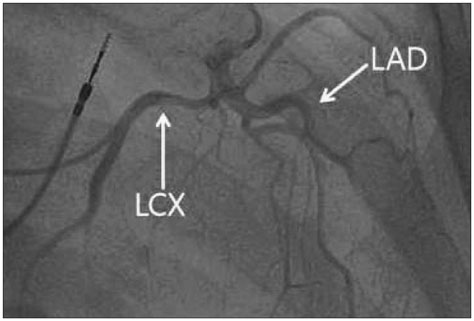
Fig. 2 Coronary angiography. There was no significant stenosis in left coronary arteries. Right coronary artery could not be examined due to failure of catheter engagement. LAD: left anterior descending artery, LCX: left circumflex artery.
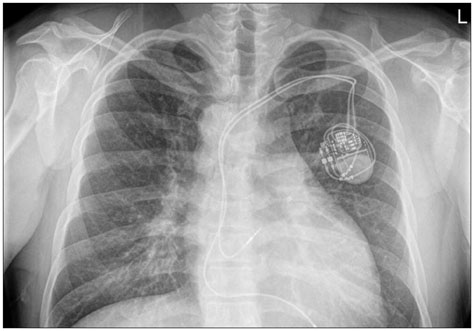
Fig. 3 Chest X-ray after permanent pacemaker insertion. A lead was positioned at RA, and V lead was positioned at functional RV (morphologic LV). Right sided aortic arch was also identified. RA: right atrium, RV: right ventricle, LV: left ventricle.
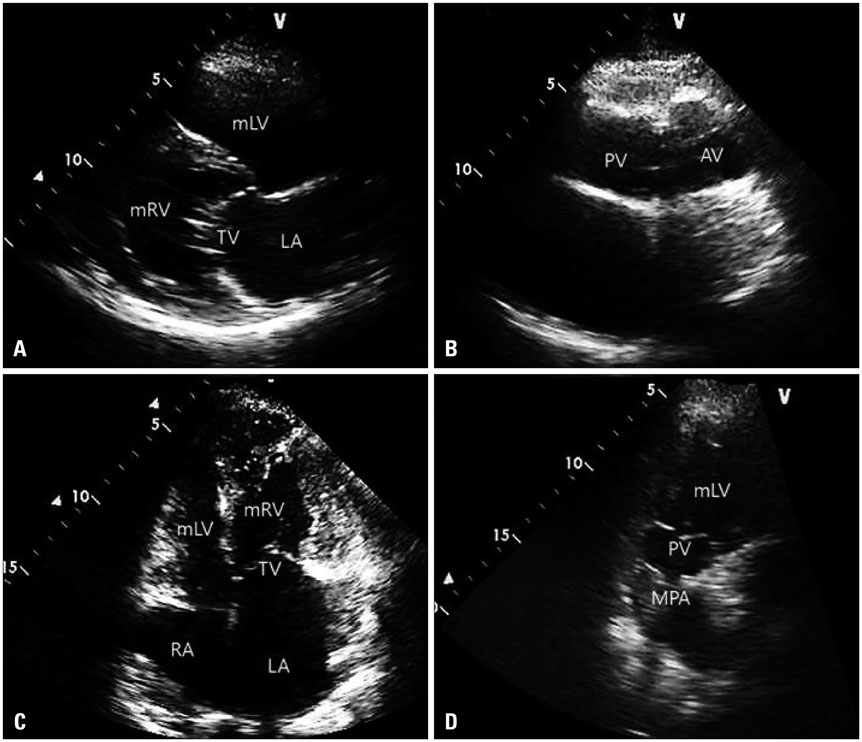
Fig. 4 Transthoracic echocardiography. Parasternal long axis view (A), parasternal short axis view (B), apical four chamber view (C), right ventricular outflow view (D). mRV was located at systemic location and mLV at pulmonary circulation. Note PV and AV location was inverted at short axis view (B). Left-sided atrioventricular valve is inferiorly located closer to the cardiac apex than right-sided atrioventricular valve (C). AV: aortic valve, LA: left atrium, mLV: morphologic left ventricle, MPA: main pulmonary artery, mRV: morphologic right ventricle, PV: pulmonary valve, RA: right atrium, TV: tricuspid valve.
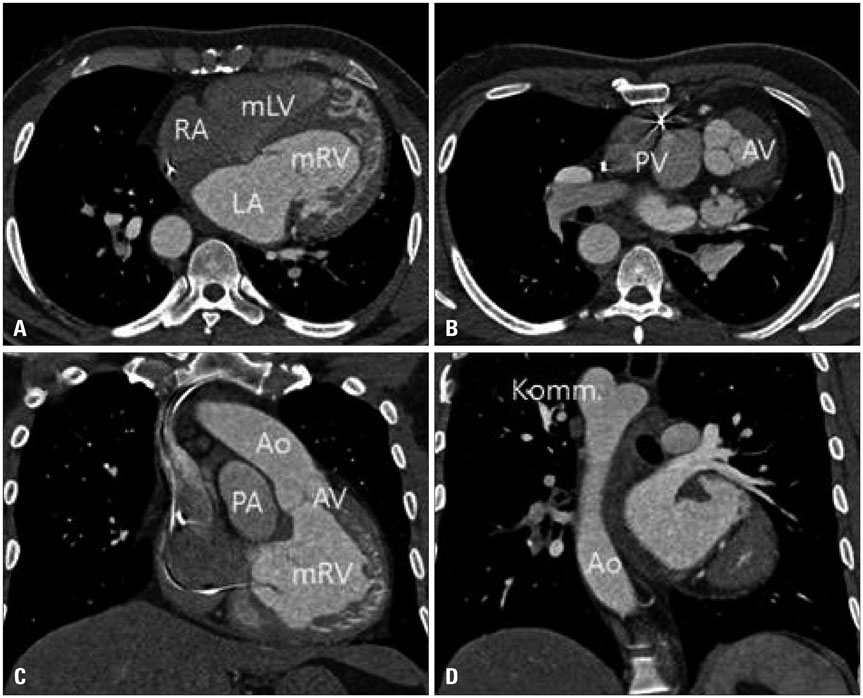
Fig. 5 Cardiac computed tomography, left-sided mRV has moderator band, coarse trabeculations (A). Aortic valve was abnormally located anterior, superior, and to the left of the pulmonic valve. Aorta arises anterior and leftward of pulmonary artery from the mRV (B and C). Right sided descending thoracic aorta with diverticulum of Kommerell (D). Ao: aorta, AV: aortic valve, Komm: diverticulum of Kommerell, LA: left atrium, mLV: morphologic left ventricle, mRV: morphologic right ventricle, PA: pulmonary artery, PV: pulmonary valve, RA: right atrium.
Reference
-
1. Warnes CA. Transposition of the great arteries. Circulation. 2006; 114:2699–2709.2. Hornung TS, Calder L. Congenitally corrected transposition of the great arteries. Heart. 2010; 96:1154–1161.3. Anderson RH, Becker AE, Arnold R, Wilkinson JL. The conducting tissues in congenitally corrected transposition. Circulation. 1974; 50:911–923.4. Wilkinson JL, Smith A, Lincoln C, Anderson RH. Conducting tissues in congenitally corrected transposition with situs inversus. Br Heart J. 1978; 40:41–48.5. Graham TP Jr, Bernard YD, Mellen BG, Celermajer D, Baumgartner H, Cetta F, Connolly HM, Davidson WR, Dellborg M, Foster E, Gersony WM, Gessner IH, Hurwitz RA, Kaemmerer H, Kugler JD, Murphy DJ, Noonan JA, Morris C, Perloff JK, Sanders SP, Sutherland JL. Long-term outcome in congenitally corrected transposition of the great arteries: a multi-institutional study. J Am Coll Cardiol. 2000; 36:255–261.6. Presbitero P, Somerville J, Rabajoli F, Stone S, Conte MR. Corrected transposition of the great arteries without associated defects in adult patients: clinical profile and follow up. Br Heart J. 1995; 74:57–59.7. Beauchesne LM, Warnes CA, Connolly HM, Ammash NM, Tajik AJ, Danielson GK. Outcome of the unoperated adult who presents with congenitally corrected transposition of the great arteries. J Am Coll Cardiol. 2002; 40:285–290.8. Prieto LR, Hordof AJ, Secic M, Rosenbaum MS, Gersony WM. Progressive tricuspid valve disease in patients with congenitally corrected transposition of the great arteries. Circulation. 1998; 98:997–1005.9. Kilner PJ. Imaging congenital heart disease in adults. Br J Radiol. 2011; 84(Spec No 3):S258–S268.10. Hauser M, Bengel FM, Hager A, Kuehn A, Nekolla SG, Kaemmerer H, Schwaiger M, Hess J. Impaired myocardial blood flow and coronary flow reserve of the anatomical right systemic ventricle in patients with congenitally corrected transposition of the great arteries. Heart. 2003; 89:1231–1235.11. Murtuza B, Barron DJ, Stumper O, Stickley J, Eaton D, Jones TJ, Brawn WJ. Anatomic repair for congenitally corrected transposition of the great arteries: a single-institution 19-year experience. J Thorac Cardiovasc Surg. 2011; 142:1348–1357.e1.12. Hraska V, Duncan BW, Mayer JE Jr, Freed M, del Nido PJ, Jonas RA. Long-term outcome of surgically treated patients with corrected transposition of the great arteries. J Thorac Cardiovasc Surg. 2005; 129:182–191.13. Rutledge JM, Nihill MR, Fraser CD, Smith OE, McMahon CJ, Bezold LI. Outcome of 121 patients with congenitally corrected transposition of the great arteries. Pediatr Cardiol. 2002; 23:137–145.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of isolated congenitally corrected transposition of the great arteries with complete atrioventricular block
- Transposition of the Great Arteries: Historical Background
- Recent Issues of Complex Transposition of the Great Arteries
- A Case Report of Congenitally Corrected Transposition of Great Arteries: Morphologic and Functional Evaluation with Cardiac CT
- A Case of Hyperthyroidism with Complete Atrioventricular Block and Cardiac Arrest
