Clin Exp Otorhinolaryngol.
2012 Sep;5(3):156-160. 10.3342/ceo.2012.5.3.156.
Intersession Repeatability of Acoustic Rhinometry Measurements in Healthy Volunteers
- Affiliations
-
- 1Academic Unit of Respiratory Medicine, UCL Medical School, London, UK. alahmari87@hotmail.com
- KMID: 2134599
- DOI: http://doi.org/10.3342/ceo.2012.5.3.156
Abstract
OBJECTIVES
Acoustic rhinometry is a rapid, reliable and non-invasive technique for the evaluation of conditions associated with impaired nasal patency. This study aimed to examine the intersession repeatability of acoustic rhinometry measurements of unilateral and combined nasal parameters in a group of healthy volunteers.
METHODS
Twenty healthy volunteers were studied. In each subject, acoustic rhinometry measurements were performed on five consecutive days, with multiple recordings. Five clinically relevant parameters were measured in each session and the intersession repeatability of these measurements was expressed in terms of mean coefficient of variation, intraclass correlation coefficient and inter-item correlations.
RESULTS
Intraclass correlation coefficients showed a high, and greater repeatability over time for all the combined (mean) values compared to the unilateral values. All intraclass correlations for combined values were > or =0.80 confirming almost perfect agreement. All intraclass correlations and inter-item correlations were associated with P<0.001. The mean coefficient of variation was low (<10%) for all but the proximal minimum cross sectional area (MCA1) measurements.
CONCLUSION
Acoustic rhinometry provides highly repeatable measurements of nasal patency, which is best for combined (mean) nasal parameters. This property makes it suitable for use in the diagnosis and follow-up of conditions associated with nasal obstruction, either structural or functional.
Figure
-
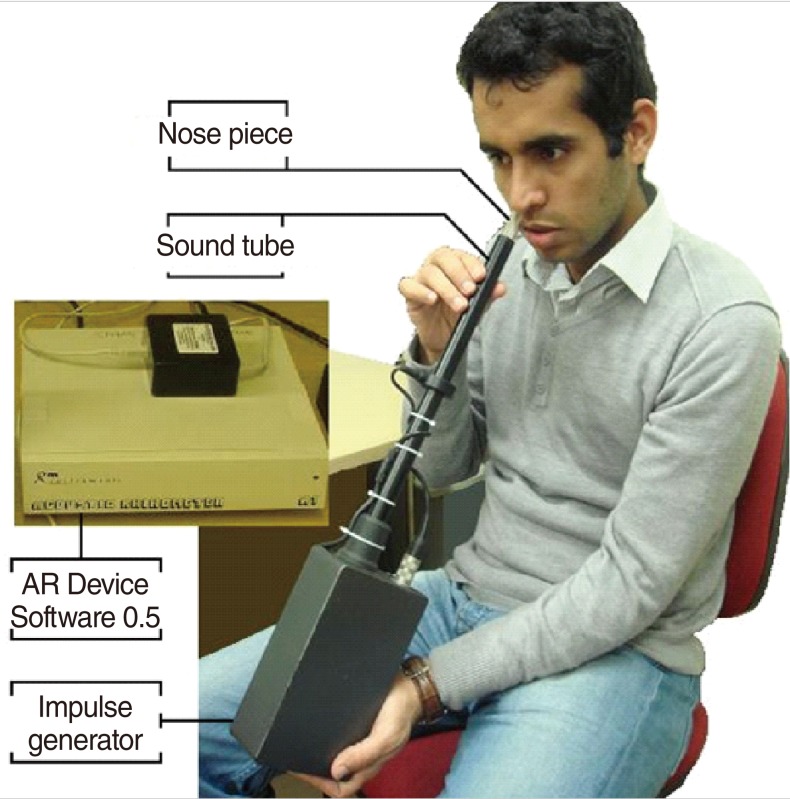
Fig. 1 Handling and positioning of the device by the subject. Reproduced with the permission of the volunteer.
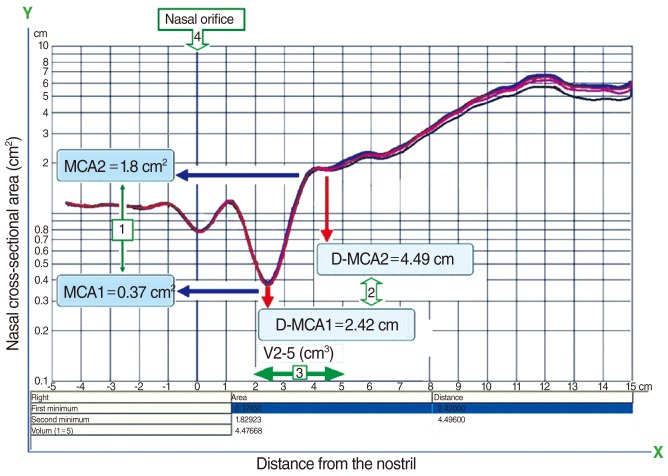
Fig. 2 An example acoustic rhimonetry trace.The x-axis represents distance from the nostril (at 0 cm), and the y-axis represents the nasal cross-sectional area (cm2). MCA1 and MCA2 (arrow 1) correspond to the nasal valve and anterior half of the inferior turbinate, respectively. D-MCA1 and D-MCA2 (arrow 2) correspond to the distance of MCA1 and MCA2 from the nasal orifice (x, 0 cm) respectively. The green arrow (arrow 3) indicates the segment used for the calculation of nasal volume between 2 and 5 cm into the nose (V2-5), and arrow 4 the nasal orifice.
Reference
-
1. Hilberg O, Jackson AC, Swift DL, Pedersen OF. Acoustic rhinometry: evaluation of nasal cavity geometry by acoustic reflection. J Appl Physiol. 1989; 1. 66(1):295–303. PMID: 2917933.
Article2. Corey JP. Acoustic rhinometry: should we be using it? Curr Opin Otolaryngol Head Neck Surg. 2006; 2. 14(1):29–34. PMID: 16467635.
Article3. Andre RF, Vuyk HD, Ahmed A, Graamans K, Nolst Trenite GJ. Correlation between subjective and objective evaluation of the nasal airway: a systematic review of the highest level of evidence. Clin Otolaryngol. 2009; 12. 34(6):518–525. PMID: 20070760.4. Cakmak O, Tarhan E, Coskun M, Cankurtaran M, Celik H. Acoustic rhinometry: accuracy and ability to detect changes in passage area at different locations in the nasal cavity. Ann Otol Rhinol Laryngol. 2005; 12. 114(12):949–957. PMID: 16425563.
Article5. Cankurtaran M, Celik H, Coskun M, Hizal E, Cakmak O. Acoustic rhinometry in healthy humans: accuracy of area estimates and ability to quantify certain anatomic structures in the nasal cavity. Ann Otol Rhinol Laryngol. 2007; 12. 116(12):906–916. PMID: 18217510.
Article6. Cheung EJ, Citardi MJ, Fakhri S, Cain J, Batra PS, Luong A. Comparison of optical rhinometry to acoustic rhinometry using nasal provocation testing with Dermatophagoides farinae. Otolaryngol Head Neck Surg. 2010; 8. 143(2):290–293. PMID: 20647137.
Article7. Corey JP, Gungor A, Nelson R, Fredberg J, Lai V. A comparison of the nasal cross-sectional areas and volumes obtained with acoustic rhinometry and magnetic resonance imaging. Otolaryngol Head Neck Surg. 1997; 10. 117(4):349–354. PMID: 9339795.
Article8. Hopkins C. Re: Correlation between subjective and objective evaluation of the nasal airway. Clin Otolaryngol. 2010; 4. 35(2):147–148. PMID: 20500587.
Article9. Munoz-Cano R, Salvador R, Valero A, Berenguer J, Alobid I, Bartra J, et al. Accuracy of acoustic rhinometry versus computed tomography in the evaluation of nasal cavity in patients with nasal polyposis. Rhinology. 2010; 6. 48(2):224–227. PMID: 20502765.
Article10. Ouriques DM, Carlini D, Fujita R, Pignatari SS, Weckx LL. Correlation between fiberoptic nasal endoscopy and acoustic rhinometry in adults without nasal complaints. Am J Rhinol. 2006; Jul-Aug. 20(4):375–378. PMID: 16955763.
Article11. Terheyden H, Maune S, Mertens J, Hilberg O. Acoustic rhinometry: validation by three-dimensionally reconstructed computer tomographic scans. J Appl Physiol. 2000; 9. 89(3):1013–1021. PMID: 10956345.
Article12. Gilain L, Coste A, Ricolfi F, Dahan E, Marliac D, Peynegre R, et al. Nasal cavity geometry measured by acoustic rhinometry and computed tomography. Arch Otolaryngol Head Neck Surg. 1997; 4. 123(4):401–405. PMID: 9109788.
Article13. Tarhan E, Coskun M, Cakmak O, Celik H, Cankurtaran M. Acoustic rhinometry in humans: accuracy of nasal passage area estimates, and ability to quantify paranasal sinus volume and ostium size. J Appl Physiol. 2005; 8. 99(2):616–623. PMID: 15802371.
Article14. Numminen J, Ahtinen M 3rd, Huhtala H, Laranne J, Rautiainen M. Correlation between rhinometric measurement methods in healthy young adults. Am J Rhinol. 2002; Jul-Aug. 16(4):203–208. PMID: 12222945.
Article15. Castano R, Theriault G, Gautrin D, Ghezzo H, Trudeau C, Malo JL. Reproducibility of acoustic rhinometry in the investigation of occupational rhinitis. Am J Rhinol. 2007; Jul-Aug. 21(4):474–477. PMID: 17882918.
Article16. Harar RP, Kalan A, Kenyon GS. Improving the reproducibility of acoustic rhinometry in the assessment of nasal function. ORL J Otorhinolaryngol Relat Spec. 2002; Jan-Feb. 64(1):22–25. PMID: 11891393.
Article17. Ognibene NE, Merrick MA, Ingersoll CD. Intra- and intersession reliability of acoustic rhinometry in measuring nasal cross-sectional area. Ear Nose Throat J. 2001; 8. 80(8):536539–540. PMID: 11523471.
Article18. Silkoff PE, Chakravorty S, Chapnik J, Cole P, Zamel N. Reproducibility of acoustic rhinometry and rhinomanometry in normal subjects. Am J Rhinol. 1999; Mar-Apr. 13(2):131–135. PMID: 10219442.
Article19. Roithmann R, Cole P, Chapnik J, Zamel N. Beproducibility of acoustic rhinometric measurements. Am J Rhinol. 1995; Sep-Oct. 9(5):263–267.20. Kesavanathan J, Swift DL, Fitzgerald TK, Permutt T, Bascom R. Evaluation of acoustic rhinometry and posterior rhinomanometry as tools for inhalation challenge studies. J Toxicol Environ Health. 1996; 6. 48(3):295–307. PMID: 8656451.
Article21. Hilberg O, Pedersen OF. Acoustic rhinometry: recommendations for technical specifications and standard operating procedures. Rhinol Suppl. 2000; 12. 16:3–17. PMID: 11225287.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Repeatability of a Multi-segment Foot Model with a 15-Marker Set in Normal Children
- Measurement of the so-called "Nasal Valve" in Japanese Subjects
- Change in the Nasal Patency and Mucociliary Clearance after Phenylephrine Spray
- Development of a Device Equipped with a Thermocouple for Measuring Nasal Airflow
- The Effects of Alcohol on Nasal Patency and Mucociliary Clearance
