Pancreatic Pseudocyst after Endoscopic Ultrasound-Guided Fine Needle Aspiration of Pancreatic Mass
- Affiliations
-
- 1Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea. jkryu@snu.ac.kr
Abstract
- Endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) is well known as a safe diagnostic procedure. We report the first case of pancreatic pseudocyst after EUS-FNA of the pancreatic body mass. A 60-year-old male underwent EUS-FNA for incidentally detected pancreatic solid mass which was suspected as neuroendocrine tumor. Two weeks later, the patient visited emergency room with acute abdominal pain and right upper quadrant tenderness; leukocytosis and elevated C-reactive protein, amylase, and lipase levels were noted. Computed tomography discovered newly developed 11.5x9.5 cm sized cystic mass communicating with the main pancreatic duct. Cyst fluid analysis revealed amylase level of 3,423 U/L and fluid culture isolated Streptococcus parasanguinis. The cystic mass corresponds with pancreatic pseudocyst. FNA induced main pancreatic duct injury and fluid leakage may cause it. Endoscopists who perform EUS-FNA must remember that pancreatic main duct injury can occur as one of severe complications and that it could be treated successfully with endoscopic internal drainage.
MeSH Terms
Figure
-
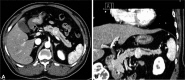
Fig. 1 Initial contrast enhanced abdominal computed tomography scan. (A) Transverse section. (B) Coronal reconstruction image. There are 2.4×2.2 cm sized slightly enhancing mass in the pancreas body portion. Main pancreatic duct of both proximal and distal side of the mass was dilated.

Fig. 2 Linear endoscopic ultrasound (GF-UCT240) which shows pancreatic body mass and passage of 22-gauge needle (EchoTip Ultra, ECHO-22). Fine needle aspiration was performed via transgastric approach and three passes were made.
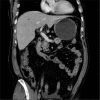
Fig. 3 Follow-up contrast enhanced abdominal computed tomography scan. A newly developed 11.5×9.5 cm sized cystic mass is observed between the stomach and the pancreas. Communication is seen between the pseudocyst and the dilated pancreatic main duct.
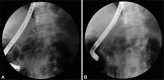
Fig. 4 Endoscopic retrograde pancreatogram. (A) Pancreatogram showed the leakage of dye from the pancreatic duct of the body portion (white arrow), and (B) transpapillary internal drainage using 7 Fr, 15 cm straight plastic stent (Percuflex Amsterdam Single-use Biliary Stents) was performed.

Fig. 5 (A) Histological image of the resected pancreatic mass showing pseudocyst and organizing hematoma in the cyst cavity (H&E stain, ×400). (B) Adjacent fat necrosis was also seen (H&E stain, ×400).
Reference
-
1. Itoi T, Sofuni A, Itokawa F, Irisawa A, Khor CJ, Rerknimitr R. Current status of diagnostic endoscopic ultrasonography in the evaluation of pancreatic mass lesions. Dig Endosc. 2011; 23(Suppl 1):17–21. PMID: 21535194.
Article2. Yoshinaga S, Suzuki H, Oda I, Saito Y. Role of endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) for diagnosis of solid pancreatic masses. Dig Endosc. 2011; 23(Suppl 1):29–33. PMID: 21535197.
Article3. O'Toole D, Palazzo L, Arotçarena R, et al. Assessment of complications of EUS-guided fine-needle aspiration. Gastrointest Endosc. 2001; 53:470–474. PMID: 11275888.4. Carrara S, Arcidiacono PG, Mezzi G, Petrone MC, Boemo C, Testoni PA. Pancreatic endoscopic ultrasound-guided fine needle aspiration: complication rate and clinical course in a single centre. Dig Liver Dis. 2010; 42:520–523. PMID: 19955025.
Article5. Williams DB, Sahai AV, Aabakken L, et al. Endoscopic ultrasound guided fine needle aspiration biopsy: a large single centre experience. Gut. 1999; 44:720–726. PMID: 10205212.
Article6. Eloubeidi MA, Tamhane A, Varadarajulu S, Wilcox CM. Frequency of major complications after EUS-guided FNA of solid pancreatic masses: a prospective evaluation. Gastrointest Endosc. 2006; 63:622–629. PMID: 16564863.
Article7. Reddymasu S, Oropeza-Vail MM, Williamson S, Jafri F, Olyaee M. Pancreatic leak after endoscopic ultrasound guided fine needle aspiration managed by transpapillary pancreatic duct stenting. JOP. 2011; 12:489–490. PMID: 21904078.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endoscopic Ultrasound-Guided Fine Needle Aspiration in Cystic Pancreatic Lesions
- Role of Repeated Endoscopic Ultrasound-Guided Fine Needle Aspiration for Inconclusive Initial Cytology Result
- Endoscopic Ultrasound-Guided Direct Intervention for Solid Pancreatic Tumors
- How to optimize the diagnostic yield of endoscopic ultrasoundguided fine-needle sampling in solid pancreatic lesions from a technical perspective
- How Can We Get the Best Results with Endoscopic Ultrasound-Guided Fine Needle Aspiration?
