Transantral Orbital Floor Fracture Repair Using a Folded Silastic Tube
- Affiliations
-
- 1Department of Otolaryngology-Head and Neck Surgery, Kosin University College of Medicine, Busan, Korea. entkwon@hanmail.net
- KMID: 2117520
- DOI: http://doi.org/10.3342/ceo.2015.8.3.250
Abstract
OBJECTIVES
The purpose of this study was to evaluate the advantages and limitations of using a silicon tube to support the fractured orbital floor by a transantral approach.
METHODS
A retrospective study was conducted from January 2000 to December. 2011 in 51 patients with pure orbital floor fractures. The patients underwent reduction surgery via a transantral approach for inserting a folded silastic tube to support the fractured orbital floor in the maxillary sinus. A chart review of preoperative and postoperative ocular symptoms, operation records, and complications was maintained.
RESULTS
In 18 out of 25 patients with diplopia, postoperative improvement was seen. In 13 out of 15 patients with extraocular muscle limitation, postoperative improvement was seen. Enophthalmos resolved postoperatively in four of five patients. Postsurgical complications occurred in three patients: an overcorrection, an infection in the maxillary sinus, and an implant extrusion, all of which were resolved by revision surgeries.
CONCLUSION
During the course of the study, we sensed reduction using a folded silastic tube via a transantral approach as an easy and effective technique with good postoperative results, and minimal implant related complications. This novel procedure is recommended as a surgical option for the reduction of orbital floor fractures.
MeSH Terms
Figure
-
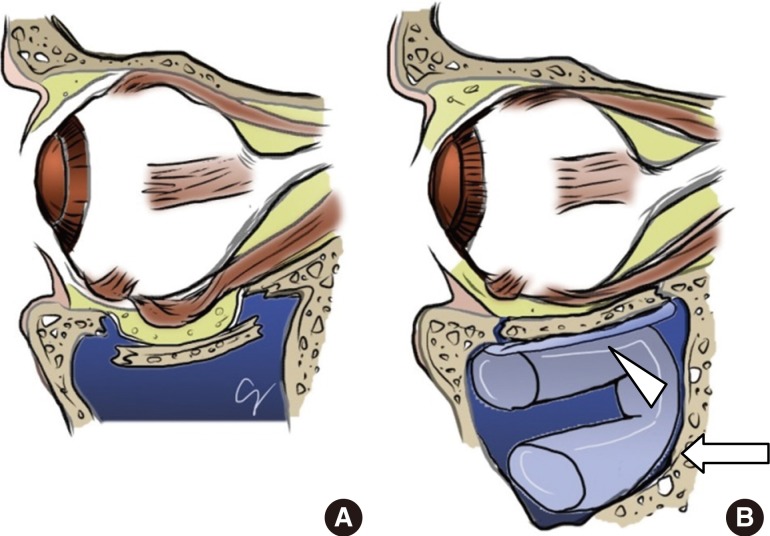
Fig. 1 Illustrations showing the repair of the orbital floor fracture. (A) Note that the fractured fragments of the orbital floor and orbital fat are returned to their original place before the insertion of implants. (B) A silastic sheet (1 mm; arrowhead) is placed under the orbital floor and a bent silicon tube (arrow) is inserted into the maxillary sinus under the silastic sheet via a transantral approach.
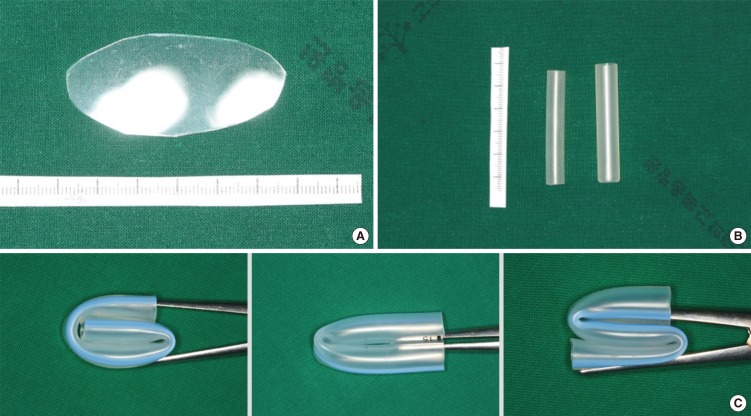
Fig. 2 Silastic sheet and tubes used in this technique. (A) Silastic sheet (1 mm in thickness) placed under the fractured orbital floor in the maxillary sinus through the antral window. (B) Silicon tubes (0.5 mm for children, 1 mm for adults) for upholding the fractured orbital floor. (C) Various strategies for bending the silicon tubes.
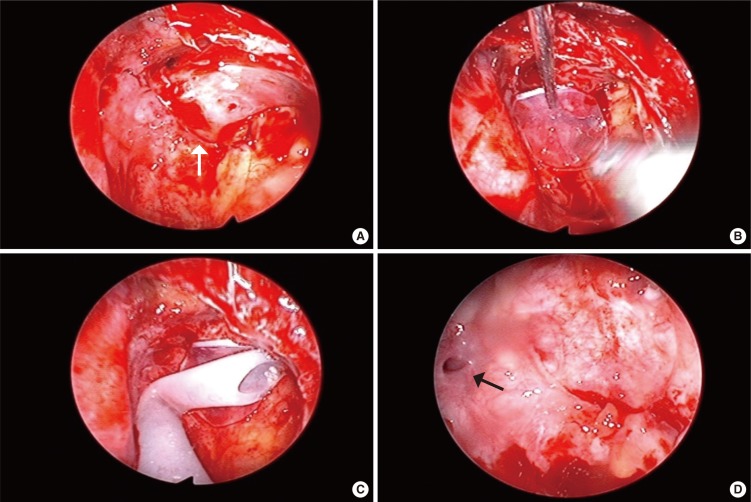
Fig. 3 Intraoperative endoscopic views of the left maxillary sinus of an orbital floor fracture, through the antral window. (A) The orbital floor was fractured, and periorbital soft tissue was herniated into the maxillary sinus (arrow). (B) The fractured orbital contents were reduced to anatomic position and a silastic sheet was placed under the fractured bone. (C) Bent silastic tubing was inserted into the maxillary sinus to support the reduced orbital floor. (D) The silastic tube and sheet were removed, and the fractured orbital floor was well reduced (arrow, natural ostium).

Fig. 4 Coronal computed tomography (CT) scans of the blowout fracture of the inferior orbital wall. (A) Preoperative view. (B) Postoperative CT scan before silicone tube removal, the inferior orbital wall was supported with the silastic sheet and silicon tube. (C) Well reduced state of fractured bony wall after removal of silicon tube, two years postsurgery.
Cited by 1 articles
-
Usefulness of Fibrin Glue in Transantral Orbital Floor Fracture Repair Using Bioresorbable Panel
Tae Jung Park, Tae Young Jung, Bo Young Kim, Seok Kim, Min Joon Kim, Jae Hwan Kwon, Kyu Sup Cho, Soo Keun Kong
Korean J Otorhinolaryngol-Head Neck Surg. 2017;60(2):69-75. doi: 10.3342/kjorl-hns.2016.16978.
Reference
-
1. Jank S, Schuchter B, Emshoff R, Strobl H, Koehler J, Nicasi A, et al. Clinical signs of orbital wall fractures as a function of anatomic location. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003; 8. 96(2):149–153. PMID: 12931086.
Article2. Manolidis S, Weeks BH, Kirby M, Scarlett M, Hollier L. Classification and surgical management of orbital fractures: experience with 111 orbital reconstructions. J Craniofac Surg. 2002; 11. 13(6):726–737. PMID: 12457084.
Article3. Lee HH, Alcaraz N, Reino A, Lawson W. Reconstruction of orbital floor fractures with maxillary bone. Arch Otolaryngol Head Neck Surg. 1998; 1. 124(1):56–59. PMID: 9440781.
Article4. Lai A, Gliklich RE, Rubin PA. Repair of orbital blow-out fractures with nasoseptal cartilage. Laryngoscope. 1998; 5. 108(5):645–650. PMID: 9591539.
Article5. Ikeda K, Suzuki H, Oshima T, Takasaka T. Endoscopic endonasal repair of orbital floor fracture. Arch Otolaryngol Head Neck Surg. 1999; 1. 125(1):59–63. PMID: 9932589.
Article6. Walter WL. Early surgical repair of blowout fracture of the orbital floor by using the transantral approach. South Med J. 1972; 10. 65(10):1229–1243. PMID: 5074094.
Article7. Gray LN, Kalimuthu R, Jayaram B, Lewis N, Sohaey M. A retrospective study of treatment of orbital floor fractures with the maxillary sinus approach. Br J Plast Surg. 1985; 1. 38(1):113–115. PMID: 3967107.
Article8. Lemke BN, Kikkawa DO. Repair of orbital floor fractures with hydroxyapatite block scaffolding. Ophthal Plast Reconstr Surg. 1999; 5. 15(3):161–165.
Article9. Folkestad L, Westin T. Long-term sequelae after surgery for orbital floor fractures. Otolaryngol Head Neck Surg. 1999; 6. 120(6):914–921. PMID: 10352449.
Article10. Converse JM, Smith B, Obear MF, Wood-Smith D. Orbital blowout fractures: a ten-year survey. Plast Reconstr Surg. 1967; 1. 39(1):20–36. PMID: 5335192.11. Courtney DJ, Thomas S, Whitfield PH. Isolated orbital blowout fractures: survey and review. Br J Oral Maxillofac Surg. 2000; 10. 38(5):496–504. PMID: 11010781.
Article12. Brady SM, McMann MA, Mazzoli RA, Bushley DM, Ainbinder DJ, Carroll RB. The diagnosis and management of orbital blowout fractures: update 2001. Am J Emerg Med. 2001; 3. 19(2):147–154. PMID: 11239261.
Article13. Saunders CJ, Whetzel TP, Stokes RB, Wong GB, Stevenson TR. Transantral endoscopic orbital floor exploration: a cadaver and clinical study. Plast Reconstr Surg. 1997; 9. 100(3):575–581. PMID: 9283552.
Article14. Whitehouse RW, Batterbury M, Jackson A, Noble JL. Prediction of enophthalmos by computed tomography after 'blow out' orbital fracture. Br J Ophthalmol. 1994; 8. 78(8):618–620. PMID: 7918289.
Article15. Raskin EM, Millman AL, Lubkin V, della Rocca RC, Lisman RD, Maher EA. Prediction of late enophthalmos by volumetric analysis of orbital fractures. Ophthal Plast Reconstr Surg. 1998; 1. 14(1):19–26.
Article16. Otori N, Haruna S, Moriyama H. Endoscopic endonasal or transmaxillary repair of orbital floor fracture: a study of 88 patients treated in our department. Acta Otolaryngol. 2003; 8. 123(6):718–723. PMID: 12953771.
Article17. Persons BL, Wong GB. Transantral endoscopic orbital floor repair using resorbable plate. J Craniofac Surg. 2002; 5. 13(3):483–488. PMID: 12040223.
Article18. Ortiz Monasterio F, Rodriguez A, Benavides A. A simple method for the correction of enophthalmos. Clin Plast Surg. 1987; 1. 14(1):169–175. PMID: 3816033.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Simultaneous Transconjunctival and Transantral Approach for Repair of Blowout Fracture by using Medpor Orbital Implant
- 2 Cases of Reduction of Orbital Floor Fracture Using Fibrin Glue for Securing Bioresorbable Panel
- Reduction of the Blowout Fracture of the Inferior Orbital Wall Using Elasticity of Silicon Tube
- Orbital Floor Fracture Reduction Via Prelacrimal Approach
- The Endoscopic Treatment of Blow-out Fracture
