Chronic Recurrent Multifocal Osteomyelitis on the Distal Tibia and Fibula
- Affiliations
-
- 1Department of Orthopedic Surgery, Busan Paik Hospital, Inje University College of Medicine, Busan, Korea. ortho1@hanmail.net
- 2Medical Department of 3821th Unit, Korea Army, Inje, Korea.
- 3Department of Interanl Medcine, Busan Paik Hospital, Inje University College of Medicine, Busan, Korea.
- KMID: 2106753
- DOI: http://doi.org/10.4055/jkoa.2015.50.2.160
Abstract
- Chronic recurrent multifocal osteomyelitis (CRMO) is a non-infectious inflammatory bone disease that occurs mainly in children and adolescents. The clinical presentation shows imprecise bone pain, while radiologic findings and histologic exam are similar to those of infectious osteomyelitis. It is a rare disease, which is difficult to distinguish from other diseases, therefore it could be misdiagnosed. We report on a case of CRMO on the distal tibia and fibula in an 11-year-old boy.
Figure
-

Figure 1 Chronic recurrent multifocal osteomyelitis in the ankle of an 11-year-old boy. (A) Anterior-posterior plain radiography of the right ankle shows an osteolytic lesion of the physeal plate at the distal fibula. (B) Coronal T2 weighted magnetic resonance imaging shows an increased signal change around the distal fibula and a periosteal reaction.
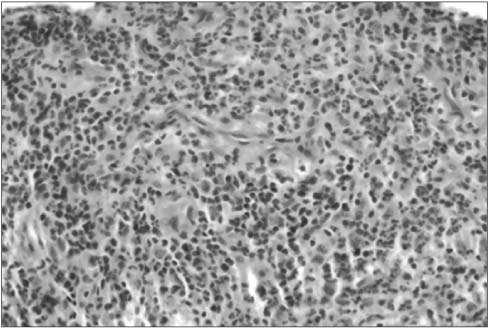
Figure 2 Histologic feature shows mixed infiltration of inflammatory cells including polymorphonuclear leukocytes, lymphocytes, and plasma cells (H&E, ×400).

Figure 3 Three months postoperative, anterior-posterior plain radiograph of the right ankle shows disappearance of the osteolytic lesion.

Figure 4 (A) Anterior-posterior plain radiograph of the right ankle shows an osteolytic lesion on the physeal plate at the distal tibia. (B) 99-mTcWhite blood cell scan shows no definite evidence of abnormal radioactivity suggesting an infectious lesion. (C) Anterior-posterior plain radiograph of the right ankle shows a reduction in the osteolytic lesion after six months.
Reference
-
1. Giedion A, Holthusen W, Masel LF, Vischer D. Subacute and chronic "symmetrical" osteomyelitis. Ann Radiol (Paris). 1972; 15:329–342.2. Iyer RS, Thapa MM, Chew FS. Chronic recurrent multifocal osteomyelitis: review. AJR Am J Roentgenol. 2011; 196:S87–S91.3. Davies AM, Grimer R. The penumbra sign in subacute osteomyelitis. Eur Radiol. 2005; 15:1268–1270.
Article4. Cho DY, Hahm YG, Kim JW. Chronic recurrent multifocal osteomyelitis: a case report. J Korean Orthop Assoc. 1996; 31:920–927.
Article5. Chung YK, Song BY, Chung BE. Chronic recurrent multifocal osteomyelitis: a case report. J Korean Orthop Assoc. 1990; 25:1576–1579.
Article6. Lee KW, Choi YJ, Ahn HS, et al. Chronic recurrent multifocal osteomyelitis of the shoulder: a case report. Clin Shoulder Elbow. 2011; 14:248–252.
Article7. Jansson A, Renner ED, Ramser J, et al. Classification of non-bacterial osteitis: retrospective study of clinical, immunological and genetic aspects in 89 patients. Rheumatology (Oxford). 2007; 46:154–160.
Article8. Schultz C, Holterhus PM, Seidel A, et al. Chronic recurrent multifocal osteomyelitis in children. Pediatr Infect Dis J. 1999; 18:1008–1013.
Article9. Ferguson PJ, Sandu M. Current understanding of the pathogenesis and management of chronic recurrent multifocal osteomyelitis. Curr Rheumatol Rep. 2012; 14:130–141.
Article10. Catalano-Pons C, Comte A, Wipff J, et al. Clinical outcome in children with chronic recurrent multifocal osteomyelitis. Rheumatology (Oxford). 2008; 47:1397–1399.
Article
