J Korean Orthop Assoc.
2011 Feb;46(1):73-77. 10.4055/jkoa.2011.46.1.73.
Spontaneously Regressed Bilateral Scapulothoracic Bursitis
- Affiliations
-
- 1Department of Orthopaedic Surgery, School of Medicine and Hospital, Gyeongsang National University, Jinju, Korea. hbinpark@gnu.ac.kr
- 2Department of Radiology, Korea General Hospital, Jinju, Korea.
- KMID: 2106575
- DOI: http://doi.org/10.4055/jkoa.2011.46.1.73
Abstract
- Scapulothoracic bursitis causes snapping scapular syndrome, which is characterized by shoulder pain accompanying bony crepitation during shoulder motion, or as an isolated entity causing shoulder discomfort. The pathogenesis of scapulothoracic bursa formation is thought to be related to chronic repetitive mechanical stress on the periscapular tissue, usually from the result of a bone abnormality (a protrusion of the scapula or rib cage). Scapulothracic bursitis is treated with conservative management and the result can be successful. Accurate diagnosis is important because surgery is not necessary except for cases with pain, excessive friction, or dysfunction. We report a patient with rapidly developed bilateral scapulothoracic bursitis without pain and snapping, which can be confused with a soft tissue sarcoma. In this case, conservative management was used to treat the patient.
Keyword
Figure
-

Figure 1 Clinical photograph shows the large bilateral masses below the inferior angles of both scapulae.
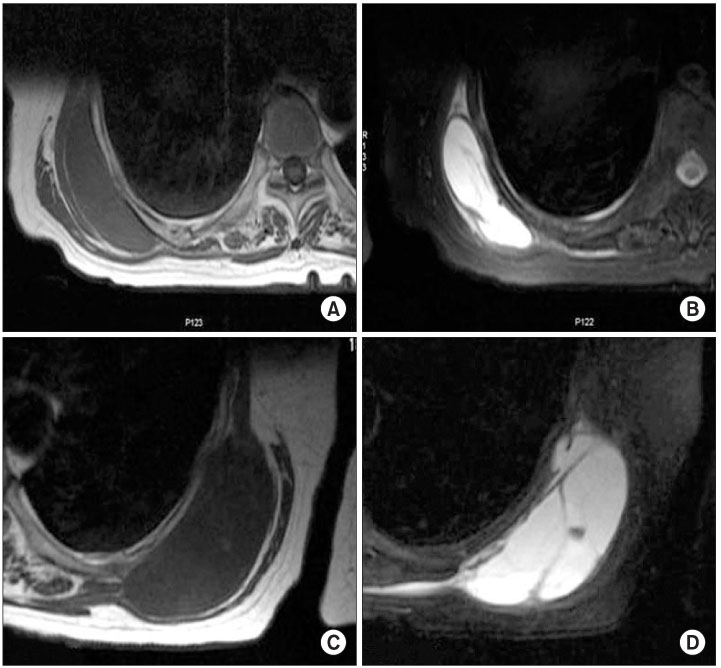
Figure 2 MR images demonstrate the well-circumscribed cystic masses located between the serratus anterior and the chest wall. The right-side cystic mass, which measures approximately 10 cm × 5.5 cm × 4 cm, demonstrates homogeneous low signal intensity on T1-weighted images (A), and homogeneous high signal intensity on T2-weighted images (B). The left-side cystic mass, which measures 10 cm × 4 cm × 3.2 cm, demonstrates homogeneous low signal intensity on T1-weighted images (C), and homogeneous high signal intensity on T2-weighted images (D).
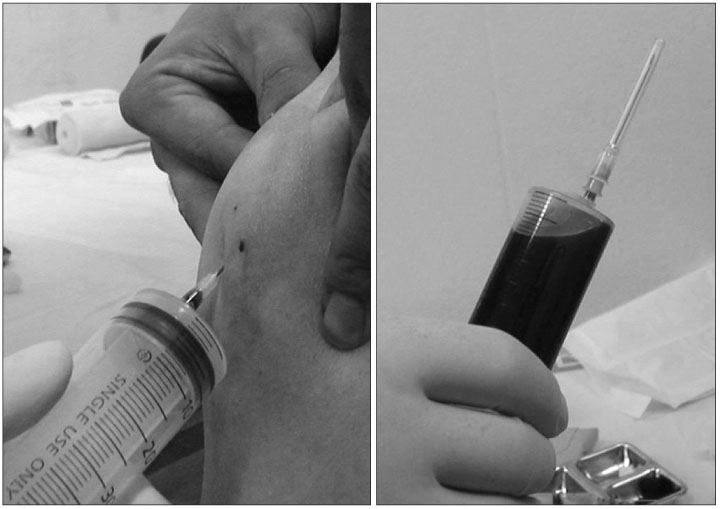
Figure 3 A diagnostic aspiration indicates that the cystic fluid is blood.
Reference
-
1. Kuhn JE, Plancher KD, Hawkins RJ. Symptomatic scapulothoracic crepitus and bursitis. J Am Acad Orthop Surg. 1998. 6:267–273.
Article2. Nicholson GP, Duckworth MA. Scapulothoracic bursectomy for snapping scapula syndrome. J Shoulder Elbow Surg. 2002. 11:80–85.
Article3. Ruland LJ 3rd, Ruland CM, Matthews LS. Scapulothoracic anatomy for the arthroscopist. Arthroscopy. 1995. 11:52–56.
Article4. Sisto DJ, Jobe FW. The operative treatment of scapulothoracic bursitis in professional pitchers. Am J Sports Med. 1986. 14:192–194.
Article5. Williams GR Jr, Shakil M, Klimkiewicz J, Iannotti JP. Anatomy of the scapulothoracic articulation. Clin Orthop Relat Res. 1999. 359:237–246.
Article6. Higuchi T, Ogose A, Hotta T, et al. Clinical and imaging features of distended scapulothoracic bursitis: spontaneously regressed pseudotumoral lesion. J Comput Assist Tomogr. 2004. 28:223–228.7. Shackcloth MJ, Page RD. Scapular osteochondroma with reactive bursitis presenting as a chest wall tumour. Eur J Cardiothorac Surg. 2000. 18:495–496.
Article8. Gross JL, Younes RN, Haddad FJ, Deheinzelin D, Pinto CA, Costa ML. Soft-tissue sarcomas of the chest wall: prognostic factors. Chest. 2005. 127:902–908.9. Zembsch A, Schick S, Trattnig S, Walter J, Amann G, Ritschl P. Elastofibroma dorsi. Study of two cases and magnetic resonance imaging findings. Clin Orthop Relat Res. 1999. 364:213–219.10. Haykir R, Karakose S, Karabacakoglu A. Elastofibroma dorsi: typical radiological features. Australas Radiol. 2007. 51 Spec No.:B95–B97.
Article11. Kourda J, Ayadi-Kaddour A, Merai S, Hantous S, Miled KB, Mezni FE. Bilateral elastofibroma dorsi. A case report and review of the literature. Orthop Traumatol Surg Res. 2009. 95:383–387.
Article12. Laffan EE, Ngan BY, Navarro OM. Pediatric soft-tissue tumors and pseudotumors: MR imaging features with pathologic correlation: part 2. Tumors of fibroblastic/myofibroblastic, so-called fibrohistiocytic, muscular, lymphomatous, neurogenic, hair matrix, and uncertain origin. Radiographics. 2009. 29:e36.13. Arkun R, Memis A, Akalin T, Ustun EE, Sabah D, Kandiloglu G. Liposarcoma of soft tissue: MRI findings with pathologic correlation. Skeletal Radiol. 1997. 26:167–172.
Article14. Schiavon F, Ragazzi R. Bilateral scapulothoracic bursitis. Arthritis Rheum. 2008. 58:585.
