J Korean Orthop Assoc.
2011 Feb;46(1):10-17. 10.4055/jkoa.2011.46.1.10.
Anatomic Reconstruction of the Lateral Ankle Instability Using the Semitendinosus Allograft Tendon and Interference Screws
- Affiliations
-
- 1Department of Orthopaedic Surgery, Konkuk University Medical Center, Seoul, Korea. jungfoot@hanmail.net
- KMID: 2106566
- DOI: http://doi.org/10.4055/jkoa.2011.46.1.10
Abstract
- PURPOSE
To evaluate the clinical outcome of the anatomic reconstruction of the lateral ankle instability using the semitendinosus allograft tendon and the interference screws.
MATERIALS AND METHODS
This study is based on the 12 feet of lateral ankle instability that had been treated with anatomic reconstruction of the anterior talofibular ligament (ATFL) and calcaneofibular ligament (CFL) using the semitendinosus allograft tendon and the interference screws. The majority of patients were young and physically active. We evaluated the patients' VAS pain scores, AOFAS scores and Karlsson-Peterson ankle scores for the 11 feet involved with at least 12 months follow up, both pre- and post-operative. In addition, we evaluated patient satisfaction. We measured the talar tilt angles and the talar anterior translations from ankle stress views.
RESULTS
The average age at surgery was 25.9 years old (19-57 years); patients had symptoms of recurrent sprain for average 31.4 months before surgery. The average follow up period was 14 months. For reconstruction, we used 4.0mm thick allograft semitendinosus tendon and interference screws. VAS pain scores decreased from 6.0 to 1.1 (p<0.05) and AOFAS scores improved from 70.4 to 90.4 postoperatively (p<0.05). Karlsson-Peterson ankle scores improved significantly from 54.6 to 92.4 (p<0.05). Radiographic talar tilt decreased from 15.7degrees to 3.2degrees postoperatively (p<0.05). Eighy-two percent of the patients were satisfied with the results and the patients had returned to their jobs by 3.7 months after surgery.
CONCLUSION
Anatomic reconstruction of the ATFL and the CFL in the lateral ankle instability patients using the semitendinosus tendon and the interference screws is an ideal surgical option especially for young athletes with high grade instabilities.
Keyword
MeSH Terms
Figure
-
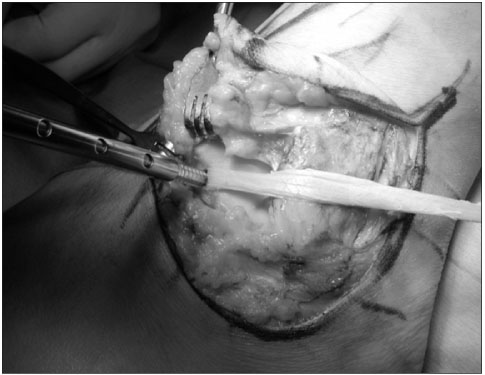
Figure 1 The semitendinosus allograft tendon was fixed with an interference screw at ATFL insertion site of anterior margin of lateral talar body.

Figure 2 Two fibular tunnels were made at ATFL and CFL attachment sites of distal fibula.
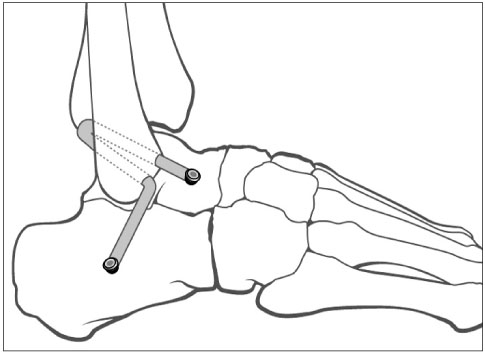
Figure 3 Schematic diagram of ATFL and CFL anatomic reconstruction with the semitendinosus allograft tendon and interference screws.
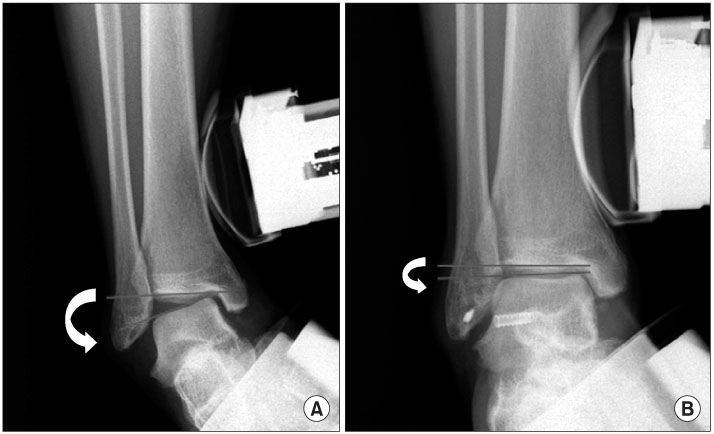
Figure 4 Varus stress radiograph of patient #6. Preoperative talar tilt of 17° (A) decreased to 3° at postoperative 18 months (B).
Reference
-
1. Colville MR. Surgical treatment of the unstable ankle. J Am Acad Orthop Surg. 1998. 6:368–377.
Article2. Colville MR, Marder RA, Boyle JJ, Zarins B. Strain measurement in lateral ankle ligaments. Am J Sports Med. 1990. 18:196–200.
Article3. Meyer JM, Garcia J, Hoffmeyer P, Fritschy D. The subtalar sprain. A roentgenographic study. Clin Orthop Relat Res. 1988. (226):169–173.4. Sammarco VJ. Complications of lateral ankle ligament reconstruction. Clin Orthop Relat Res. 2001. (391):123–132.
Article5. Caprio A, Oliva F, Treia F, Maffulli N. Reconstruction of the lateral ankle ligaments with allograft in patients with chronic ankle instability. Foot Ankle Clin. 2006. 11:597–605.
Article6. Broström L. Sprained ankles. VI. Surgical treatment of "chronic" ligament ruptures. Acta Chir Scand. 1966. 132:551–565.7. Gould N, Seligson D, Gassman J. Early and late repair of lateral ligament of the ankle. Foot Ankle. 1980. 1:84–89.
Article8. Ahlgren O, Larsson S. Reconstruction for lateral ligament injuries of the ankle. J Bone Joint Surg Br. 1989. 71:300–303.
Article9. Karlsson J, Bergsten T, Lansinger O, Peterson L. Surgical treatment of chronic lateral instability of the ankle joint. A new procedure. Am J Sports Med. 1989. 17:268–273.10. Girard P, Anderson RB, Davis WH, Isear JA, Kiebzak GM. Clinical evaluation of the modified Brostrom-Evans procedure to restore ankle stability. Foot Ankle Int. 1999. 20:246–252.
Article11. Evans DL. Recurrent instability of the ankle; a method of surgical treatment. Proc R Soc Med. 1953. 46:343–344.12. Chrisman OD, Snook GA. Reconstruction of lateral ligament tears of the ankle. An experimental study and clinical evaluation of seven patients treated by a new modification of the Elmslie procedure. J Bone Joint Surg Am. 1969. 51:904–912.13. Watson-Jones R. Fractures and joint injuries. 1955. 4th ed. Edinburgh: E & S Livingstone Ltd.14. Rosenbaum D, Bertsch C, Claes LE. NOVEL Award 1996: 2nd prize Tenodeses do not fully restore ankle joint loading characteristics: a biomechanical in vitro investigation in the hind foot. Clin Biomech (Bristol, Avon). 1997. 12:202–209.15. Kjaersgaard-Andersen P, Søjbjerg JO, Wethelund JO, Helmig P, Madsen F. Watson-Jones tenodesis for ankle instability. A mechanical analysis in amputation specimens. Acta Orthop Scand. 1989. 60:477–480.16. Kjaersgaard-Andersen P, Madsen F, Frich LH, Wethelund JO, Søjbjerg JO. Lateral hindfoot instability treated with the Evans tenodesis: a biomechanical analysis. J Foot Surg. 1990. 29:25–32.17. Paterson R, Cohen B, Taylor D, Bourne A, Black J. Reconstruction of the lateral ligaments of the ankle using semi-tendinosis graft. Foot Ankle Int. 2000. 21:413–419.
Article18. Sugimoto K, Takakura Y, Kumai T, Iwai M, Tanaka Y. Reconstruction of the lateral ankle ligaments with bone-patellar tendon graft in patients with chronic ankle instability: a preliminary report. Am J Sports Med. 2002. 30:340–346.19. Coughlin MJ, Schenck RC Jr, Grebing BR, Treme G. Comprehensive reconstruction of the lateral ankle for chronic instability using a free gracilis graft. Foot Ankle Int. 2004. 25:231–241.
Article20. Kitaoka HB, Alexander IJ, Adelaar RS, Nunley JA, Myerson MS, Sanders M. Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int. 1994. 15:349–353.
Article21. Karlsson J, Peterson L. Evaluation of ankle joint function: the use of a scoring scale. Foot (Edinb). 1991. 1:15–19.
Article22. Elmslie RC. Recurrent subluxation of the ankle-joint. Ann Surg. 1934. 100:364–367.23. Krips R, van Dijk CN, Halasi PT, et al. Long-term outcome of anatomical reconstruction versus tenodesis for the treatment of chronic anterolateral instability of the ankle joint: a multicenter study. Foot Ankle Int. 2001. 22:415–421.
Article24. Karlsson J, Eriksson BI, Bergsten T, Rudholm O, Swärd L. Comparison of two anatomic reconstructions for chronic lateral instability of the ankle joint. Am J Sports Med. 1997. 25:48–53.
Article25. Bell SJ, Mologne TS, Sitler DF, Cox JS. Twenty-six-year results after Broström procedure for chronic lateral ankle instability. Am J Sports Med. 2006. 34:975–978.
Article26. Becker HP, Rosenbaum D, Zeithammel G, et al. Tenodesis versus carbon fiber repair of ankle ligaments: a clinical comparison. Clin Orthop Relat Res. 1996. (325):194–202.27. Jeys L, Korrosis S, Stewart T, Harris NJ. Bone anchors or interference screws? A biomechanical evaluation for autograft ankle stabilization. Am J Sports Med. 2004. 32:1651–1659.28. Burks RT, Morgan J. Anatomy of the lateral ankle ligaments. Am J Sports Med. 1994. 22:72–77.
Article29. Marrale J, Morrissey MC, Haddad FS. A literature review of autograft and allograft anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2007. 15:690–704.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Lateral Ankle Ligament Reconstruction using Achilles Allograft for Chronic failed Instability: Two Cases Report
- Indications of Lateral Ankle Ligament Reconstruction with a Free Tendon and Associated Evidence
- Chronic Lateral Ankle Instability
- Surgical Treatment of Chronic Ankle Lateral Instability: Reconstruction with Tenodesis or Tendon Graft
- Surgical Treatment of Chronic Lateral Ankle Instability: Repair versus Reconstruction
