Diagnostic Value of Multidetector Computed Tomography in Radial Head or Neck Fractures
- Affiliations
-
- 1Department of Radiology, School of Medicine, Ewha Womans University, Mokdong Hospital, Seoul, Korea. mshjy@ewha.ac.kr
- 2Department of Orthopaedic Surgery, School of Medicine, Ewha Womans University, Mokdong Hospital, Seoul, Korea.
- KMID: 2097984
- DOI: http://doi.org/10.3348/jksr.2012.67.6.473
Abstract
- PURPOSE
To evaluate the diagnostic value of multidetector computed tomography (MDCT) in radial head or neck fracture, and to evaluate factors that affect MDCT image quality.
MATERIALS AND METHODS
Sixty-six radial fractures in 65 patients, who underwent both radiography and MDCT, were included. Detection of fracture and classification of types were recorded for each modality. Patients were divided into the good (A) and poor (B) image quality groups, and recorded the factors, such as arm positioning, flexion angle, and cancellous bone density.
RESULTS
The detection rate of fracture showed no significant difference between the two modalities. However, classification of the fracture type was significantly accurate by MDCT (p < 0.0001). Eight cases were only detected on MDCT and three cases were only detected on radiography. Fracture type was discordant in 11 cases. MDCT scanning with raising arm (p < 0.0001), with lesser flexion angle (p = 0.004), and higher cancellous bone density (p = 0.010) showed better image quality.
CONCLUSION
Radiography is a good primary tool for detecting radial head or neck fracture. However, MDCT can be an additional tool for classifying the fracture type and cases with negative radiographic findings. Arm positioning, flexion angle, and cancellous bone density affect MDCT image quality.
Figure
-
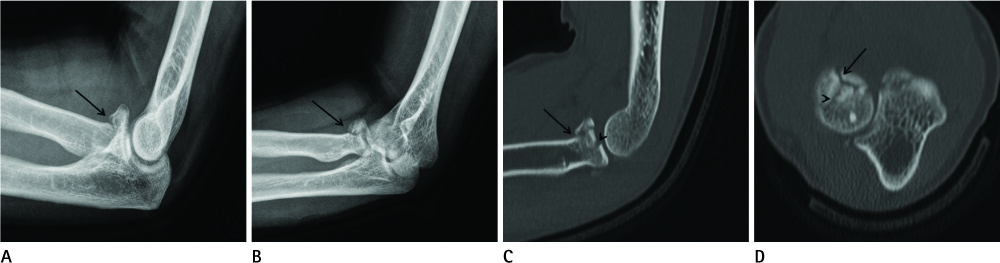
Fig. 1 Type III radial fracture in 38-year-old man. On lateral (A) and external oblique (B) views, fracture with 2.5 mm displacement is noted (arrow), diagnosed as Type II fracture. On sagittal (C) and axial (D) planes of multidetector computed tomography, another fracture line (arrowhead) is seen with displacement, diagnosed as Type III fracture. Articular depression is better depicted on sagittal plane (C) than axial plane (D).
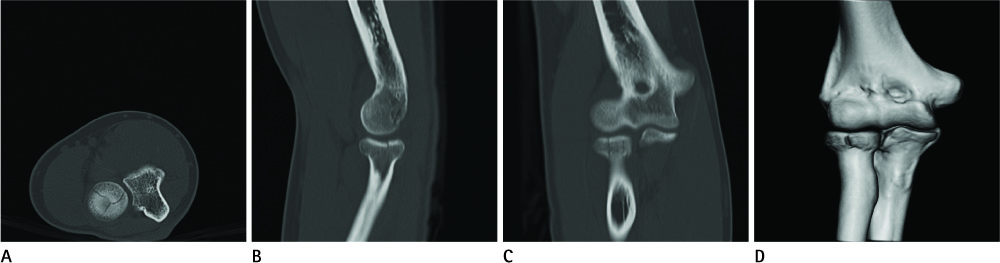
Fig. 2 Type III radial fracture in 28-year-old man (Group A). The fracture lines are clearly noted on axial (A), sagittal (B), coronal (C) planes and volume rendering technique image (D). In this case, patient positioned with raising his arm, flexion angle of elbow joint was 30° and cancellous bone density of radius was measured about 360 Hounsfield unit.

Fig. 3 Type I radial fracture in 56-year-old woman (Group B). The fracture lines are not seen on axial (A), sagittal (B) and coronal (C) planes. Volume rendering technique image (D) is non-diagnostic due to disturbance artifacts. In this case, patient was positioned with lowering her arm, with flexion angle about 70° and cancellous bone density was lower than 200 HU. Fracture line at the radial head was detected on anterior posterior view of radiography (E).
Reference
-
1. Broberg MA, Morrey BF. Results of delayed excision of the radial head after fracture. J Bone Joint Surg Am. 1986; 68:669–674.2. Pike JM, Athwal GS, Faber KJ, King GJ. Radial head fractures--an update. J Hand Surg Am. 2009; 34:557–565.3. Tejwani NC, Mehta H. Fractures of the radial head and neck: current concepts in management. J Am Acad Orthop Surg. 2007; 15:380–387.4. Karlsson MK, Herbertsson P, Nordqvist A, Besjakov J, Josefsson PO, Hasserius R. Comminuted fractures of the radial head. Acta Orthop. 2010; 81:224–227.5. Neumann M, Nyffeler R, Beck M. Comminuted fractures of the radial head and neck: is fixation to the shaft necessary. J Bone Joint Surg Br. 2011; 93:223–228.6. Matsunaga FT, Tamaoki MJ, Cordeiro EF, Uehara A, Ikawa MH, Matsumoto MH, et al. Are classifications of proximal radius fractures reproducible. BMC Musculoskelet Disord. 2009; 10:120.7. Pappas N, Bernstein J. Fractures in brief: radial head fractures. Clin Orthop Relat Res. 2010; 468:914–916.8. Dillon MT, Getz CL, Beredjiklian PK, Wiesel BB, Carolan GF, Ramsey ML. Evaluation of reliability of the Mason classification for radial head fractures. Am J Orthop (Belle Mead NJ). 2010; 39:430–443.9. Welling RD, Jacobson JA, Jamadar DA, Chong S, Caoili EM, Jebson PJ. MDCT and radiography of wrist fractures: radiographic sensitivity and fracture patterns. AJR Am J Roentgenol. 2008; 190:10–16.10. Guy RL, Butler-Manuel PA, Holder P, Brueton RN. The role of 3D CT in the assessment of acetabular fractures. Br J Radiol. 1992; 65:384–389.11. Chapman V, Grottkau B, Albright M, Elaini A, Halpern E, Jaramillo D. MDCT of the elbow in pediatric patients with posttraumatic elbow effusions. AJR Am J Roentgenol. 2006; 187:812–817.12. Bahrs C, Rolauffs B, Südkamp NP, Schmal H, Eingartner C, Dietz K, et al. Indications for computed tomography (CT-) diagnostics in proximal humeral fractures: a comparative study of plain radiography and computed tomography. BMC Musculoskelet Disord. 2009; 10:33.13. Hughes SS, Voit G, Kates SL. The role of computerized tomography in the diagnosis of an occult femoral neck fracture associated with an ipsilateral femoral shaft fracture: case report. J Trauma. 1991; 31:296–298.14. Draffan D, Clements D, Farrell M, Heller J, Bennett D, Carmichael S. The role of computed tomography in the classification and management of pelvic fractures. Vet Comp Orthop Traumatol. 2009; 22:190–197.15. McAdams TR, Blevins FT, Martin TP, DeCoster TA. The role of plain films and computed tomography in the evaluation of scapular neck fractures. J Orthop Trauma. 2002; 16:7–11.16. Philipp MO, Kubin K, Mang T, Hörmann M, Metz VM. Three-dimensional volume rendering of multidetector-row CT data: applicable for emergency radiology. Eur J Radiol. 2003; 48:33–38.17. Polacin A, Kalender WA, Marchal G. Evaluation of section sensitivity profiles and image noise in spiral CT. Radiology. 1992; 185:29–35.18. Polacin A, Kalender WA, Brink J, Vannier MA. Measurement of slice sensitivity profiles in spiral CT. Med Phys. 1994; 21:133–140.19. McCollough CH, Zink FE. Performance evaluation of a multi-slice CT system. Med Phys. 1999; 26:2223–2230.20. Droege RT, Morin RL. A practical method to measure the MTF of CT scanners. Med Phys. 1982; 9:758–760.21. McNitt-Gray MF. AAPM/RSNA Physics Tutorial for Residents: Topics in CT. Radiation dose in CT. Radiographics. 2002; 22:1541–1155.22. Seibert JA. Tradeoffs between image quality and dose. Pediatr Radiol. 2004; 34:Suppl 3. S183–S195. discussion S234-S24123. Barrett JF, Keat N. Artifacts in CT: recognition and avoidance. Radiographics. 2004; 24:1679–1691.24. Siegel EL, Templeton AW, Cook LT, Eckard DA, Harrison LA, Dwyer SJ 3rd. Image calibration of laser digitizers, printers, and gray-scale displays. Radiographics. 1992; 12:329–335.25. Boyd AS, Benjamin HJ, Asplund C. Splints and casts: indications and methods. Am Fam Physician. 2009; 80:491–499.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Silicone Prosthesis Replacement for the Treatment of Radial Head Fractures
- Multidetector Computed Tomography in Patients with Femoral Neck Fracture for Assessing Osteoporosis: Comparison with Dual Energy X-Ray Absorptiometry
- Computed tomography-based analysis of the characteristics of fifth metacarpal neck fractures and its clinical applications
- Stress Fracture of Olecranon after Plate Fixation for Osteoporotic Monteggia Fracture with Absence of Radial Head: A Case Report
- Isolated Multiple Fragmented Cricoid Fracture Associated with External Blunt Neck Trauma: A Case Report
