Preoperative Conventional Magnetic Resonance Images versus Magnetic Resonance Arthrography of Subacromial Impingement Syndrome
- Affiliations
-
- 1Department of Radiology, Pusan National University Yangsan Hospital, Yangsan, Korea. tymn@pusan.ac.kr
- 2Medical Research Institute, Pusan National University Hospital, Busan, Korea.
- 3Department of Orthopedic Surgery, Pusan National University Yangsan Hospital, Yangsan, Korea.
- KMID: 2097970
- DOI: http://doi.org/10.3348/jksr.2012.67.3.187
Abstract
- PURPOSE
To evaluate the usefulness of conventional magnetic resonance images (MRI) for arthroscopic surgery in subacromial impingement syndrome of the shoulder, as an alternative to MR arthrography with additional T2 fat saturation images (MRA).
MATERIALS AND METHODS
The preoperative MRI of 77 patients (45 females, 32 males) (52 right, 25 left) and MRA of 34 patients (14 females, 20 males) (24 right, 10 left) with subsequent arthroscopic confirmation of subacromial impingement syndrome were reviewed retrospectively. The lesions requiring arthroscopic surgery were 95 subacromial spurs, 101 subacromial bursitis, and 51 full-thickness and 44 partial-thickness tears of the supraspinatus among 111 cases for both studies. A two-by-two table was constructed in order to calculate the sensitivity and specificity of both studies against arthroscopic outcomes. Also we analyzed the false positive and false negative cases of the full-thickness tears individually.
RESULTS
The detection rates of subacromial spur and bursitis and full- and partial-thickness tears of the supraspinatus were 91%, 94%, 77%, and 65% in MRI and 93%, 100%, 83%, and 77% in MRA respectively. Their specificities were 33%, 33%, 90%, and 76% in MRI and 50%, 75%, 100%, and 71% in MRA respectively. Eleven false negative cases in regards to MRI resulted in Ellman's grade 3 partial thickness tear (72.7%), mild bursitis (63.6%), greater tuberosity erosion (45.5%), and negative fluid signal of the glenohumeral joint (81.8%). Three false positive cases on the MRI were induced from errors with lower window depth and width on the imagings. Two false negative cases on MRA were induced from the adhesion between Ellman's grade 3 rim-rent tear and the glenohumeral joint cavity.
CONCLUSION
Conventional MR images could be used to decide the arthroscopic surgery in subacromial impingement syndrome, as an alternative to MR arthrography with additional T2 fat saturation images.
MeSH Terms
Figure
-

Fig. 1 56-year-old man with full-thickness tear of the supraspinatus confirmed by arthroscopy. A. Coronal oblique fat-suppressed fast spin-echo T2 weighted magnetic resonance (MR) image shows a rim-rent bursa side tear as the partial-thickness tear (thick arrow) and bony erosions in the greater tuberosity (small arrows). B. Axial fat-suppressed fast spin-echo T2 weighted MR image shows a rim-rent bursa side tear (thick arrow) and subacromial bursitis (small arrows).
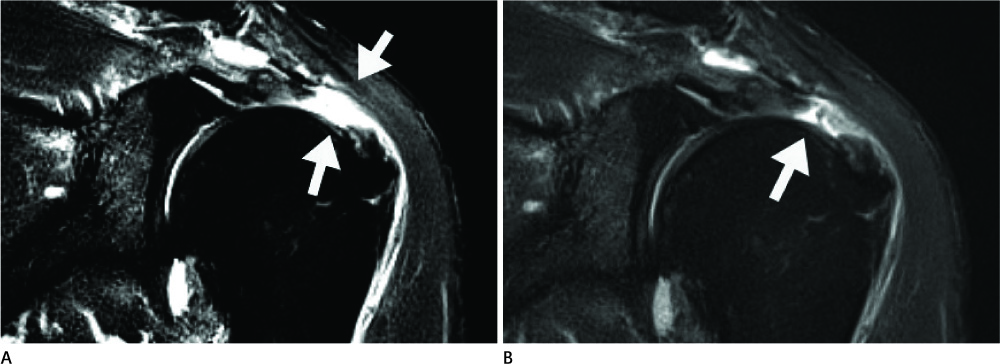
Fig. 2 57-year-old man with partial articular supraspinatus tendon avulsion confirmed by arthroscopy. A. Coronal oblique fat-suppressed fast spin-echo T2 weighted magnetic resonance (MR) image with a 614 window width and a 113 window level shows a stage 2 full-thickness tear (arrows) at the critical zone of the supraspinatus. B. The MR image corrected to a 896 window width and a 364 window level shows a partial-thickness tear (arrow).
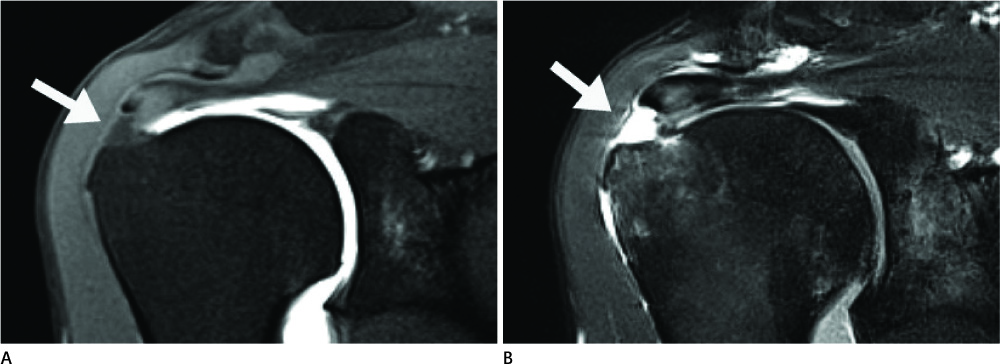
Fig. 3 51-year-old man with right shoulder subacromial impingement syndrome. A. Coronal oblique fat-suppressed fast spin-echo T1 weighted magnetic resonance (MR) arthrographic image shows no evidence of any rotator cuff injury (arrow). B. Additional coronal oblique fat-suppressed fast spin-echo T2 weighted MR arthrographic image shows a rim-rent bursa side tear (arrow) confirmed to be a full-thickness tear with adhesion.
Reference
-
1. Park HB, Yokota A, Gill HS, El Rassi G, McFarland EG. Diagnostic accuracy of clinical tests for the different degrees of subacromial impingement syndrome. J Bone Joint Surg Am. 2005. 87:1446–1455.2. MacDonald P, McRae S, Leiter J, Mascarenhas R, Lapner P. Arthroscopic rotator cuff repair with and without acromioplasty in the treatment of full-thickness rotator cuff tears: a multicenter, randomized controlled trial. J Bone Joint Surg Am. 2011. 93:1953–1960.3. Gerber C, Zubler V, Hodler J, Catanzaro S, Jost B, Fucentese SF. Dynamic imaging and function of partial supraspinatus tendon tears. Arthroscopy. 2011. 27:1180–1186.4. Chun KA, Kim MS, Kim YJ. Comparisons of the various partial-thickness rotator cuff tears on MR arthrography and arthroscopic correlation. Korean J Radiol. 2010. 11:528–535.5. Ellman H. Diagnosis and treatment of incomplete rotator cuff tears. Clin Orthop Relat Res. 1990. 64–74.6. Nam D, Maak TG, Raphael BS, Kepler CK, Cross MB, Warren RF. Rotator cuff tear arthropathy: evaluation, diagnosis, and treatment: AAOS exhibit selection. J Bone Joint Surg Am. 2012. 94:e34.7. Seitz AL, Michener LA. Ultrasonographic measures of subacromial space in patients with rotator cuff disease: a systematic review. J Clin Ultrasound. 2011. 39:146–154.8. Oh JH, Kim JY, Lee HK, Choi JA. Classification and clinical significance of acromial spur in rotator cuff tear: heel-type spur and rotator cuff tear. Clin Orthop Relat Res. 2010. 468:1542–1550.9. Vinson EN, Helms CA, Higgins LD. Rim-rent tear of the rotator cuff: a common and easily overlooked partial tear. AJR Am J Roentgenol. 2007. 189:943–946.10. Magee T. 3-T MRI of the shoulder: is MR arthrography necessary? AJR Am J Roentgenol. 2009. 192:86–92.11. Blevins FT, Djurasovic M, Flatow EL, Vogel KG. Biology of the rotator cuff tendon. Orthop Clin North Am. 1997. 28:1–16.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ankle Impingement Syndrome
- Acromial Downslping and Subacromial Interval in Shoulder Impingement Syndrome
- Anatomy, Variants, and Pathologies of the Superior Glenohumeral Ligament: Magnetic Resonance Imaging with Three-Dimensional Volumetric Interpolated Breath-Hold Examination Sequence and Conventional Magnetic Resonance Arthrography
- Magnetic Resonance Arthrography of the Shoulder Joint
- Massive Subacromial Bursitis with Rice Bodies in Rheumatoid Arthritis
