J Korean Soc Radiol.
2011 Feb;64(2):123-129. 10.3348/jksr.2011.64.2.123.
MDCT Evaluation of Left Atrium and Pulmonary Vein in the Patients with Atrial Fibrillation: Comparison with the Non-Atrial Fibrillation Group
- Affiliations
-
- 1Department of Radiology, Korea University Medical Center, Seoul, Korea. cadpel2@naver.com
- 2Department of Radiology, Korea University Guro Hospital, Seoul, Korea.
- 3Department of Biostatistics, Korea University, Seoul, Korea.
- 4Department of Cardiology, Korea University Medical Center, Seoul, Korea.
- KMID: 2097927
- DOI: http://doi.org/10.3348/jksr.2011.64.2.123
Abstract
- PURPOSE
The anatomy of the left atrium (LA) and the pulmonary veins (PVs) is important in planning and performing successful electrophysiologic ablation (EPA) for atrial fibrillation (Afib) patients. The authors estimated the findings of LA and PVs of Afib patients by MDCT, and compared these with the findings of LA and PVs of the non-Afib group using coronary CT angiography (CCTA).
MATERIALS AND METHODS
From September, 2009 to February, 2010, 91 Afib patients underwent PVCT (male: female = 72:19, mean age = 55.0-years-old) before EPA. At same time, 90 patients underwent CCTA (male: female = 73:17, mean age = 59.1-years-old). Two radiologists reviewed and analyzed all axial and 3D images of LA and PVs retrospectively with consensus.
RESULTS
The average LA volumes of the Afib group(100.49 mm3) was larger than that of the non-Afib group (78.38 mm3) (p<0.05). The average lengths of the LA right wall in the Afib group (40.25 mm) was longer than that of the non-Afib group (37.3 mm) (p<0.05). The average distances between the PV ostium and first segmental bifurcation of the Lt superior PV (LSPV) and the RSPV were shorter in the Afib group (LSPV, 19.38 mm; RSPV, 11.49 mm) than in the non-Afib group (LSPV, 23.23 mm; RSPV, 14.25 mm) (p<0.05). There were higher incidences of anomalous branches such as ostial, accessory branches, or common ostia in the Afib group versus the non-Afib group (p<0.05).
CONCLUSION
In Afib group, variable parameters of LA and PVs were obtained and estimated by MDCT, and there was statistically significant difference in the parameters of LA and PVs between Afib and non-Afib groups.
MeSH Terms
Figure
-
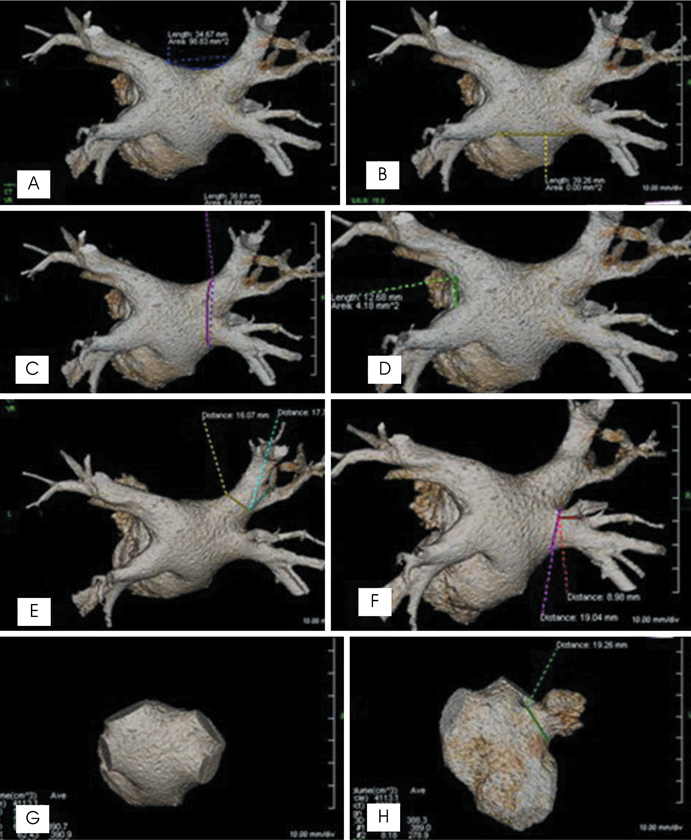
Fig. 1 Measurements of parameters in Afib group. (A) Superior roof, (B) inferior roof, (C) right lateral wall, (D) left carina, (E) and (F) ostium of PV, and diameter between ostium and first segmental bifurcation, (G) LA volume, (H) ostium of LA appendage. Volume of the ostium of the LA appendage was measured as: volume of (H) - volume of (G).
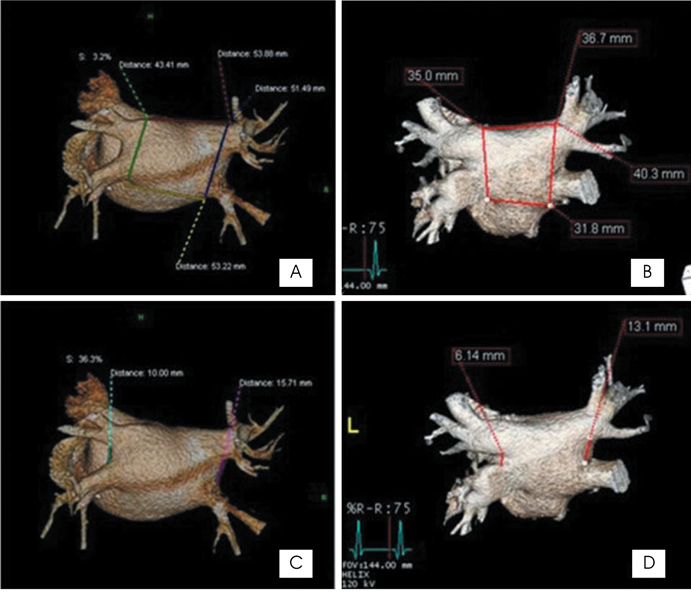
Fig. 2 Comparison of parameters in Afib group (A and C) with non-Afib group (B and D).
Reference
-
1. Stanford W, Breen JF. CT evaluation of left atrial pulmonary venous anatomy. Int J Cardiovasc Imaging. 2005; 21:133–139.2. Lacomis JM, Wigginton W, Fuhrman C, Schwartzman D, Armfield DR, Pealer KM. Multi-detector row CT of the left atrium and pulmonary veins before radio-frequency catheter ablation for atrial fibrillation. Radiographics. 2003; 23 Spec No:S35–S48.3. Tsao HM, Wu MH, Huang BH, Lee SH, Lee KT, Tai CT, et al. Morphologic remodeling of pulmonary veins and left atrium after catheter ablation of atrial fibrillation. J Ccardiovasc Electrophysiol. 2005; 16:7–12.4. Lacomis JM, Goitein O, Deible C, Schwartzman D. CT of the pulmonary veins. J Thorac Imaging. 2007; 22:63–76.5. Piorkowski C, Hindricks G, Schreiber D, Tanner H, Weise W, Koch A, et al. Electroanatomic reconstruction of the left atrium, pulmonary veins, and esophagus compared with the "true anatomy" on multislice computed tomography in patients undergoing catheter ablation of atrial fibrillation. Heart Rhythm. 2006; 3:317–327.6. Centonze M, Del Greco M, Nollo G, Ravelli F, Marini M, Della Sala SW, et al. The role of multidetector CT in the evaluation of the left atrium and pulmonary veins anatomy before and after radio-frequency catheter ablation for atrial fibrillation. Preliminary results and work in progress. Technical note. Radiol Med. 2005; 110:52–56.7. Jongbloed MR, Dirksen MS, Bax JJ, Boersma E, Geleijns K, Lamb HJ, et al. Atrial fibrillation: multi-detector row CT of pulmonary vein anatomy prior to radiofrequency catheter ablation--initial experience. Radiology. 2005; 234:702–709.8. Dittrich HC, Pearce LA, Asinger RW, Mcbride R, Webel R, Zabalgoitia M, et al. Left atrial diameter in nonvalvular atrial fibrillation: an echocardiographic study. Am Heart J. 1999; 137:494–499.9. Sanfilippo AJ, Abascal VM, Sheehan M, Oertel LB, Harrigan P, Hughes RA, et al. Atrial enlargement as a consequence of atrial fibrillation. A prospective echocardiographic study. Circulation. 1990; 82:792–797.10. Li YH, Lai LP, Shyu KG, Hwang JJ, Kuan P, Lien WP. Clinical implications of left atrial appendage flow patterns in nonrheumatic atrial fibrillation. Chest. 1994; 105:748–752.11. Verhorst PM, Kamp O, Visser CA, Verheugt FW. Left atrial appendage flow velocity assessment using transesophageal echocardiography in nonrheumatic atrial fibrillation and systemic embolism. Am J Cardiol. 1993; 71:192–196.12. Wongcharoen W, Tsao HM, Wu MH, Tai CT, Chang SL, Lin YJ, et al. Morphologic characteristics of the left atrial appendage, roof, and septum: implications for the ablation of atrial fibrillation. J Cardiovasc Electrophysiol. 2006; 17:951–956.13. Kato R, Lickfett L, Meininger G, Dickfeld T, Wu R, Juang G, et al. Pulmonary vein anatomy in patients undergoing catheter ablation of atrial fibrillation: lessons learned by use of magnetic resonance imaging. Circulation. 2003; 107:2004–2010.14. Lin WS, Prakash VS, Tai CT, Hsieh MH, Tsai CF, Yu WC, et al. Pulmonary vein morphology in patients with paroxysmal atrial fibrillation initiated by ectopic beats originating from the pulmonary veins: implications for catheter ablation. Circulation. 2000; 101:1274–1281.15. Tsao HM, Yu WC, Cheng HC, Wu MH, Tai CT, Lin WS, et al. Pulmonary vein dilation in patients with atrial fibrillation: detection by magnetic resonance imaging. J Cardiovasc Electrophysiol. 2003; 12:809–813.16. Ho SY, Sanchez-Quintana D, Cabrera JA, Anderson RH. Anatomy of the left atrium: implications for radiofrequency ablation of atrial fibrillation. J Cardiovasc Electrophysiol. 1999; 10:1525–1533.17. Chiang SJ, Tsao HM, Wu MH, Tai CT, Chang SL, Wongcharoen W, et al. Anatomic characteristics of the left atrial isthmus in patients with atrial fibrillation: lessons from computed tomographic images. J Cardiovasc Electrophysiol. 2006; 17:1274–1278.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Controlled Atrial Fibrillation after Pulmonary Vein Stenting
- Relation between Atrial Fibrillation and Echocardiographic Size of Left Atrium
- Plain chest PA evaluation of left atrial thrombosis in mitral valvular disease
- The Influence of Electrical Cardioversion for Atrial Fibrillation on Left Atrial Appendage Function: A Transesophageal Echocardiography Study
- Relation of Right Atrial Pathology to Atrial Fibrillation in Mitral Valvular Disease
