The cutoff value of saphenous vein diameter to predict reflux
- Affiliations
-
- 1Department of Surgery, Kyung Hee University Hospital at Gangdong, Kyung Hee University School of Medicine, Seoul, Korea. jhjoh@khu.ac.kr
- KMID: 2096707
- DOI: http://doi.org/10.4174/jkss.2013.85.4.169
Abstract
- PURPOSE
Increased saphenous vein diameter is a common consequence of saphenous vein reflux. Until now, there have been no reports about the correlation between diameter and reflux of saphenous vein in Korea. The aim of this study was to investigate the correlation between saphenous vein reflux and diameter changes.
METHODS
From April 2009 to August 2012, 777 patients were sent to the vascular laboratory for evaluation of venous reflux. The diameter of the saphenous vein was measured with B-mode imaging, and reflux was quantified based on valve closure time using Doppler spectral tracings. Receiver operating characteristics curve analysis was applied to determine the best saphenous vein diameter cutoff for predicting reflux.
RESULTS
The mean diameters of normal great saphenous vein (GSV) and refluxed GSV were 5.0 +/- 2.4 mm and 6.4 +/- 2.0 mm, respectively. The mean diameters of normal small saphenous vein (SSV) and refluxed SSV were 3.1 +/- 1.3 mm and 5.2 +/- 2.7 mm, respectively. The diameter differences between the normal and refluxed GSV and SSV were 1.4 mm and 2.1 mm, respectively, and these differences were statistically significant (P < 0.0001). A GSV threshold diameter of 5.05 mm had the best positive predictive value for reflux. The sensitivity and specificity at 5.05 mm were 76% and 60%, respectively. The best SSV diameter for predicting reflux was 3.55 mm. The sensitivity and specificity at 3.55 mm were 87% and 71%, respectively.
CONCLUSION
GSV diameter of > or =5.05 mm had the best positive predictive value for pathologic reflux. For pathologic reflux of SSV, the best cutoff diameter was 3.55 mm.
Keyword
MeSH Terms
Figure
-
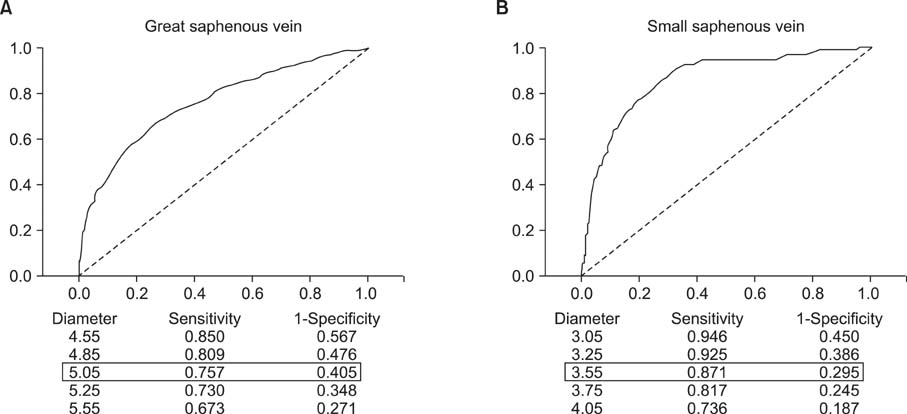
Fig. 1 Receiver operating characteristics curve analysis for determining the best cutoff value for diagnosing reflux. (A) For the great saphenous vein, 5.05 mm was the best cutoff value to predict reflux with the broadest area under the curve. (B) For the small saphenous vein, 3.55 mm was the best cutoff value to predict reflux.
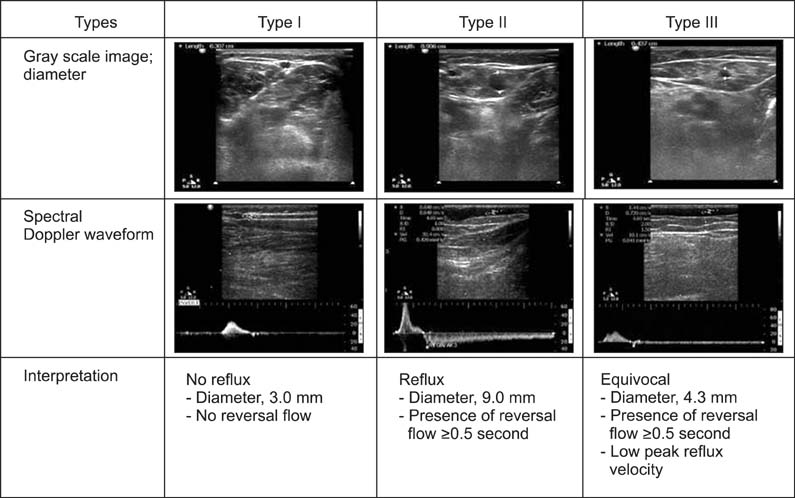
Fig. 2 Duplex findings and each interpretation for the evaluation of superficial venous insuffiency of the lower extremity. Type I is typical finding of absence of reflux; small diameter and no reversal flow. Type II is typical finding of presence of reflux; large diameter and reversal flow more than 0.5 second. Type III is equivocal finding. In spectral Doppler waveform, it shows presence of reversal flow more than 0.5 seconds with low peak reflux velocity. Diameter criteria can be used as an additional parameter in this case.
Reference
-
1. Beebe-Dimmer JL, Pfeifer JR, Engle JS, Schottenfeld D. The epidemiology of chronic venous insufficiency and varicose veins. Ann Epidemiol. 2005; 15:175–184.2. Cesarone MR, Belcaro G, Nicolaides AN, Geroulakos G, Griffin M, Incandela L, et al. 'Real' epidemiology of varicose veins and chronic venous diseases: the San Valentino Vascular Screening Project. Angiology. 2002; 53:119–130.3. Brand FN, Dannenberg AL, Abbott RD, Kannel WB. The epidemiology of varicose veins: the Framingham Study. Am J Prev Med. 1988; 4:96–101.4. Engelhorn C, Engelhorn A, Salles-Cunha S, Picheth E, Castro N Jr, Dabul N Jr, et al. Relationship between reflux and greater saphenous vein diameter. J Vasc Technol. 1997; 21:167–171.5. Mendoza E, Blattler W, Amsler F. Great saphenous vein diameter at the saphenofemoral junction and proximal thigh as parameters of venous disease class. Eur J Vasc Endovasc Surg. 2013; 45:76–83.6. Navarro TP, Delis KT, Ribeiro AP. Clinical and hemodynamic significance of the greater saphenous vein diameter in chronic venous insufficiency. Arch Surg. 2002; 137:1233–1237.7. Coleridge-Smith P, Labropoulos N, Partsch H, Myers K, Nicolaides A, Cavezzi A. Duplex ultrasound investigation of the veins in chronic venous disease of the lower limbs: UIP consensus document. Part I. Basic principles. Eur J Vasc Endovasc Surg. 2006; 31:83–92.8. Parés JO, Juan J, Tellez R, Mata A, Moreno C, Quer FX, et al. Varicose vein surgery: stripping versus the CHIVA method: a randomized controlled trial. Ann Surg. 2010; 251:624–631.9. Cappelli M, Lova RM, Ermini S, Turchi A, Bono G, Bahnini A, et al. Ambulatory conservative hemodynamic management of varicose veins: critical analysis of results at 3 years. Ann Vasc Surg. 2000; 14:376–384.10. Sarin S, Sommerville K, Farrah J, Scurr JH, Coleridge Smith PD. Duplex ultrasonography for assessment of venous valvular function of the lower limb. Br J Surg. 1994; 81:1591–1595.11. Labropoulos N, Tiongson J, Pryor L, Tassiopoulos AK, Kang SS, Ashraf Mansour M, et al. Definition of venous reflux in lower-extremity veins. J Vasc Surg. 2003; 38:793–798.12. van Bemmelen PS, Mattos MA, Hodgson KJ, Barkmeier LD, Ramsey DE, Faught WE, et al. Does air plethysmography correlate with duplex scanning in patients with chronic venous insufficiency? J Vasc Surg. 1993; 18:796–807.13. Jäger K, Seifert H, Bollinger A. M-mode echovenography: a new technique for the evaluation of venous wall and valve motion. Cardiovasc Res. 1989; 23:25–30.14. Goldman MP, Fronek A. Anatomy and pathophysiology of varicose veins. J Dermatol Surg Oncol. 1989; 15:138–145.15. Jeanneret C, Jager KA, Zaugg CE, Hoffmann U. Venous reflux and venous distensibility in varicose and healthy veins. Eur J Vasc Endovasc Surg. 2007; 34:236–242.16. Lattimer CR, Azzam M, Kalodiki E, Makris GC, Geroulakos G. Saphenous pulsation on duplex may be a marker of severe chronic superficial venous insufficiency. J Vasc Surg. 2012; 56:1338–1343.17. Murphy MA, Hands L. Is arteriovenous shunting involved in the development of varicosities? A study of the intraluminal pressure and oxygen content in varicose veins. Phlebology. 2008; 23:137–141.18. Lee W, Chung JW, Yin YH, Jae HJ, Kim SJ, Ha J, et al. Three-Dimensional CT venography of varicose veins of the lower extremity: image quality and comparison with doppler sonography. AJR Am J Roentgenol. 2008; 191:1186–1191.19. Min SK, Kim SY, Park YJ, Lee W, Jung IM, Lee T, et al. Role of three-dimensional computed tomography venography as a powerful navigator for varicose vein surgery. J Vasc Surg. 2010; 51:893–899.20. Mdez-Herrero A, Gutierrez J, Camblor L, Carreno J, Llaneza J, Rguez-Olay J, et al. The relation among the diameter of the great saphenous vein, clinical state and haemodynamic pattern of the saphenofemoral junction in chronic superficial venous insufficiency. Phlebology. 2007; 22:207–213.21. Gibson K, Meissner M, Wright D. Great saphenous vein diameter does not correlate with worsening quality of life scores in patients with great saphenous vein incompetence. J Vasc Surg. 2012; 56:1634–1641.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Prevalence and Clinical Implication of Nonsaphenous Vein Reflux with or without Pelvic Venous Disease
- Patterns of Saphenous Vein Reflux and Treatment Plan
- The Effect of Saphenous Vein Ablation on Combined Segmental Popliteal Vein Reflux
- Successful use of VenaSeal system for the treatment of large great saphenous vein of 2.84-cm diameter
- Ultrasonographic Reflux Findings of Varicose Veins of the Lower Extremities - The 2023 Korean Society for Phlebology Clinical Practice Guidelines
