Percutaneous Treatment of an Injured Coronary Stent Using the Looping Wire Technique
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Chonbuk National University Hospital, Jeonju, Korea. medorche@jbnu.ac.kr
- KMID: 2048818
- DOI: http://doi.org/10.4068/cmj.2013.49.3.129
Abstract
- Drug-eluting stent implantation is an effective treatment for coronary artery disease, yet unexpected serious complications during stent implantation are possible. A 70-year-old man with unstable angina presented with a left main bifurcation lesion. Two drug-eluting stents were successfully deployed at the left main bifurcation lesion by the mini-crush technique under intravascular ultrasound guidance. However, after removal of the wire and intravascular ultrasound catheter, the stent of the proximal left circumflex artery was damaged and shortened at the distal edge. We used a looping wire technique to cross the injured stent and we successfully re-dilated the damaged portion of the stent. Finally, we deployed an additional drug-eluting stent at the left circumflex artery over the damaged stent. Our case illustrates the importance of gentle handling of devices during coronary intervention. Furthermore, interventionists should keep in mind the role of intravascular ultrasound when treating this kind of serious complication.
Keyword
MeSH Terms
Figure
-
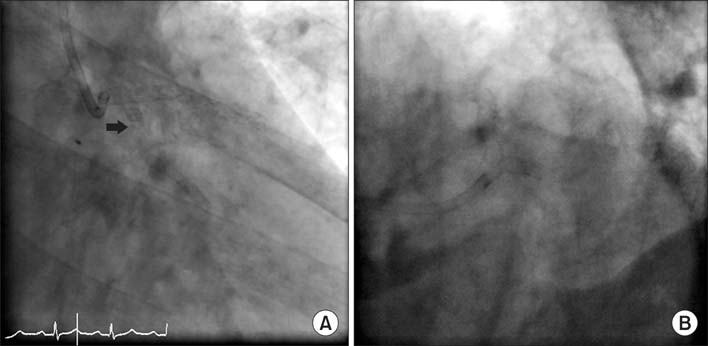
FIG. 1 Coronary angiography was done after implantation of two stents. After removal of the IVUS catheter, there was distal edge damage and shortening of the EES at the LCX in both the RAO caudal (A, black arrow) and spider view (B). IVUS: intravascular ultrasound, EES: everolimus-eluting stent, LCX: left circumflex artery, RAO: right anterior oblique.
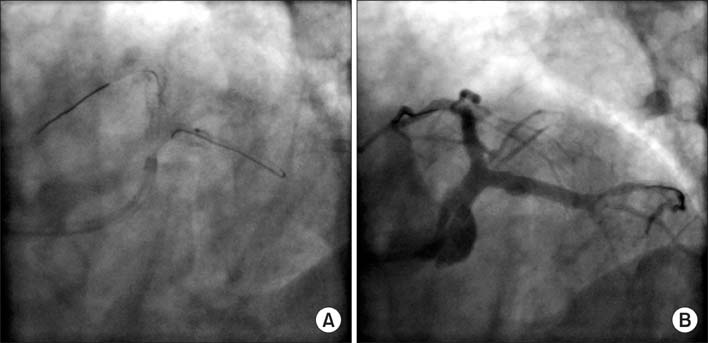
FIG. 2 We performed a looping wire technique using a 0.014'' hi-torque Balance Middleweight universal coronary guide wire (Abbott Vascular, Santa Clara, CA, USA) to cross the damaged stent and we successfully re-dilated the damaged portion (A). The final coronary angiography showed good flow with dye staining at the LCX (B). LCX: left circumflex artery.
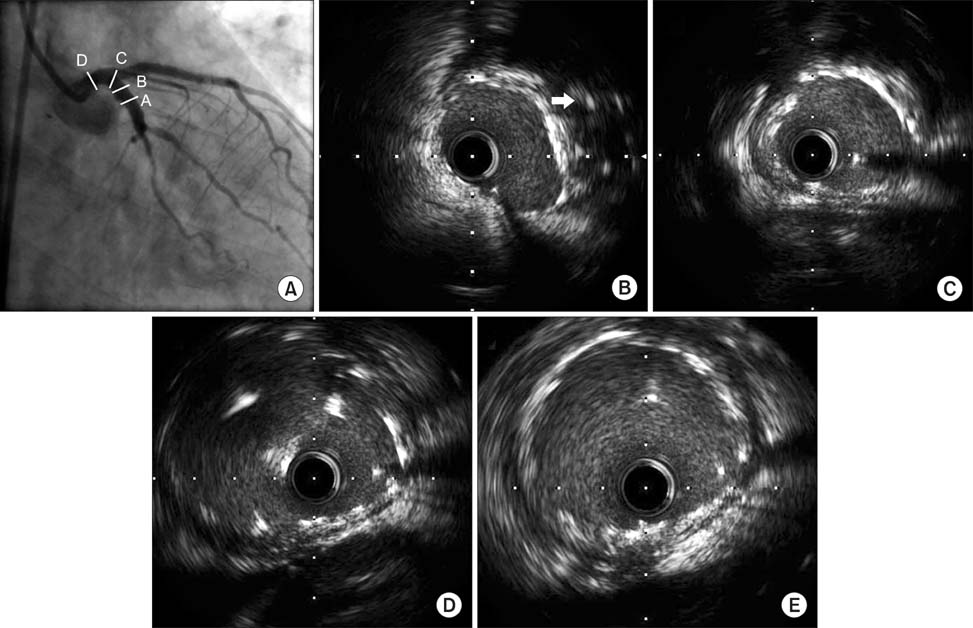
FIG. 3 Coronary angiography after EES implantation (A): IVUS finding in each point. IVUS using a pull-back system from the distal coronary artery showed good expansion and the three well-apposed EESs at the distal left main (E), the bifurcation of the left main (D), and the proximal LCX (C), with the exception of the partially crushed EES (B, white arrow). IVUS: intravascular ultrasound, EES: everolimus-eluting stent, LCX: left circumflex artery.
Reference
-
1. Williams DO, Holubkov R, Yeh W, Bourassa MG, Al-Bassam M, Block PC, et al. Percutaneous coronary intervention in the current era compared with 1985-1986: the National Heart, Lung, and Blood Institute Registries. Circulation. 2000; 102:2945–2951.
Article2. Holmes DR, Selzer F, Johnston JM, Kelsey SF, Holubkov R, Cohen HA, et al. National Heart, Lung, and Blood Institute Dynamic Registry. Modeling and risk prediction in the current era of interventional cardiology: a report from the National Heart, Lung, and Blood Institute Dynamic Registry. Circulation. 2003; 107:1871–1876.
Article3. Lee SR, Jeong MH, Ahn YK, Chae SC, Hur SH, Kim YJ, et al. Korea Acute Myocardial Infarction Registry Investigators. Clinical safety of drug-eluting stents in the Korea acute myocardial infarction registry. Circ J. 2008; 72:392–398.
Article4. Lee KH, Lee SR, Jin GY, Lee SH, Rhee KS, Chae JK, et al. Double coronary artery stent fracture with coronary artery microaneurysms. Int Heart J. 2009; 50:127–132.
Article5. Lee MS, Jurewitz D, Aragon J, Forrester J, Makkar RR, Kar S. Stent fracture associated with drug-eluting stents: clinical characteristics and implications. Catheter Cardiovasc Interv. 2007; 69:387–394.
Article6. Fang HY, Bhasin A, Youssef A, Hsueh SK, Fang CY. Intravascular ultrasound (IVUS) guided fixation of an accidentally crushed coronary stent. Int Heart J. 2008; 49:621–627.
Article7. Hong YM, Lee SR. A case of guide wire fracture with remnant filaments in the left anterior descending coronary artery and aorta. Korean Circ J. 2010; 40:475–477.
Article8. Sasseen BM, Burke JA, Shah R, Costa MA, Zenni M, Gilmore P, et al. Intravascular ultrasound catheter entrapment after coronary artery stenting. Catheter Cardiovasc Interv. 2002; 57:229–233.
Article9. Alfonso F, Flores A, Escaned J, Sanmartín M, Hernández R, Fernández-Ortíz A, et al. Pressure wire kinking, entanglement, and entrapment during intravascular ultrasound studies: a potentially dangerous complication. Catheter Cardiovasc Interv. 2000; 50:221–225.
Article10. Kim JY, Lee NH, Cho YH, Suh J, Seo HS, Kim do H, et al. Recanalization of an accidentally crushed coronary stent by intravascular ultrasonography catheter entrapment. Korean Circ J. 2011; 41:327–330.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Demystifying the Quandary of Ostial Stenting
- Treatment of Stent Dislodgement Complicated by Coronary Artery Dissection using Parallel Wire Technique and Small Balloon
- Recanalization of an Accidentally Crushed Coronary Stent by Intravascular Ultrasonography Catheter Entrapment
- Percutaneous Coronary Intervention in Ischemic Heart Disease
- Retrieval of a dislodged and dismounted coronary stent; using a rendezvous and snare technique at the brachial artery level via femoral approach
