Two Different Successful Angioplasty Methods in Patients with Stenotic Coronary Artery Ectasia
- Affiliations
-
- 1Cardiovascular Center, Korea University Guro Hospital, Seoul, Korea. swrha617@yahoo.co.kr
- KMID: 2048811
- DOI: http://doi.org/10.4068/cmj.2012.48.3.185
Abstract
- There is no current guideline for percutaneous coronary angioplasty in stenotic ectatic coronary arteries because of the heterogeneity of the coronary artery morphology. We report two successful angioplasty cases in coronary artery ectasia with different clinical scenarios. One case showed atherosclerotic stenosis in the ectatic portion of the right coronary artery that was aggravated after a coronary artery bypass graft. In this case, balloon angioplasty alone without stenting showed acceptable results at the 6-month follow-up coronary angiography. In the other case, we used a peripheral artery balloon and stent for stenosis in the ectatic portion of a large coronary artery. Six-month follow-up coronary angiography showed excellent patency of the previously implanted peripheral stent.
Keyword
MeSH Terms
Figure
-

FIG. 1 Computed tomography (CT) and invasive angiography showing the patient's abdominal aortic aneurysm in the ascending aorta and significant stenosis in the right ectatic coronary artery. The CT aortogram (A) shows both the abdominal aortic aneurysm (red arrow) and the ascending aortic aneurysm (white arrow). Coronary CT angiography (B) and right coronary angiography (C) show the focal severe stenotic lesion (white arrows) in the mid portion of the ectatic right coronary artery.
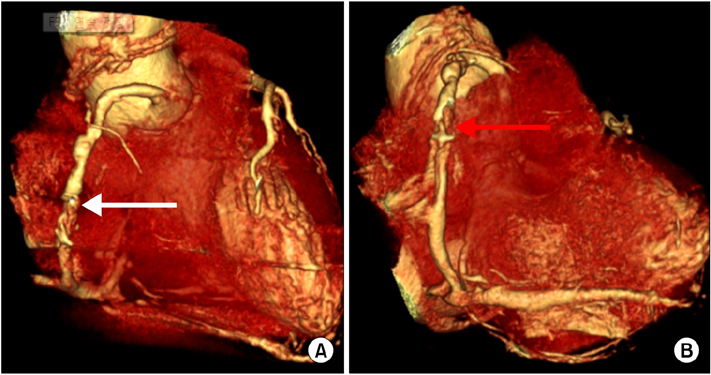
FIG. 2 Follow-up coronary CT angiography after 7 months showing two focal sites of eccentric significant stenosis (white arrow in A and red arrow in B) with soft plaque in the mid right coronary artery.
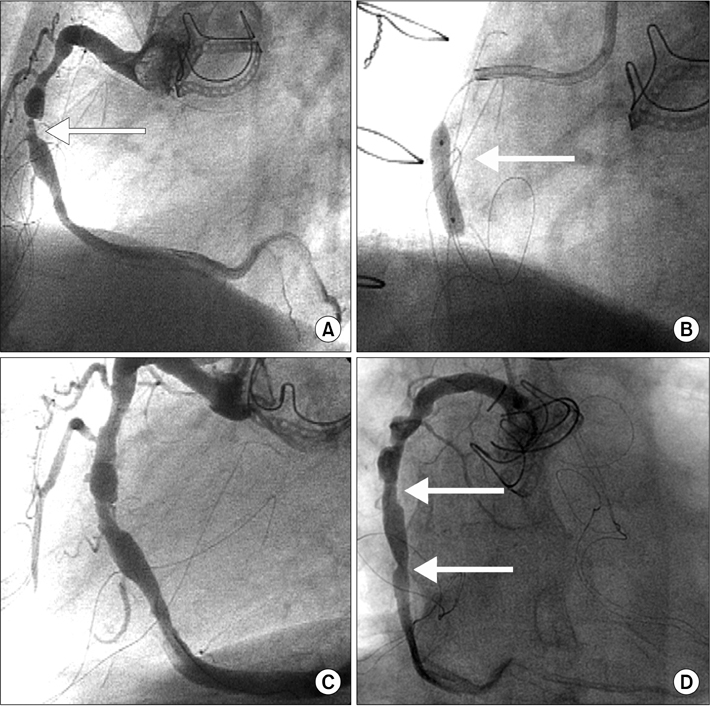
FIG. 3 Coronary angiography at baseline, during percutaneous coronary angioplasty, after percutaneous coronary angioplasty, and at follow-up. (A) Coronary angiography showing moderate tubular concentric stenosis in the proximal RCA and severe discrete concentric stenosis in the mid RCA with ectatic change. (B) Sequential balloon dilation with Avita 3.0×15 mm and Mercury 4.0×20 mm balloons was performed in the mid right coronary artery. (C) Coronary angiography after balloon angioplasty showing a well expanded stenotic lesion without flow limitation. (D) Follow-up coronary angiography after 6 months showing acceptable patency at the previous balloon angioplasty sites (white arrow).

FIG. 4 Coronary angiography and intravascular ultrasound (IVUS) image showing before, during, and after the percutaneous coronary angioplasty. (A) Baseline coronary angioplasty showing severe tubular eccentric stenosis (white arrow) in the mid left circumflex artery with ectatic change. (B) Coronary angiography showing deployment of a Genesis 6.0×24 mm stent (white arrow). (C) Coronary angiography showing a well expanded stent without flow limitation. (D) IVUS showing eccentric plaque burden (white arrow) from the 5 o'clock to the 7 o'clock direction. The reference vessel diameter just distal to the lesion was 6.2×6.8 mm on IVUS measurement. (E) Post-stenting IVUS showed good apposition and expansion of the stent.
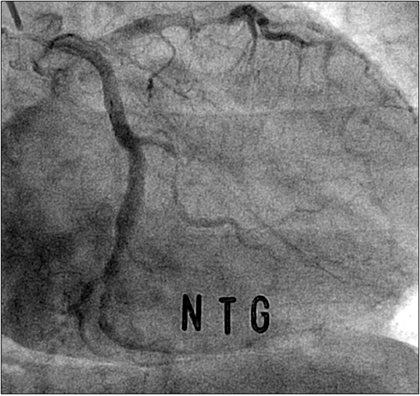
FIG. 5 Follow-up coronary angiography at 6 months showing the previous stent to be patent without significant in-stent restenosis.
Cited by 1 articles
-
ST-Segment Elevation Myocardial Infarction as a Result of Coronary Artery Ectasia-Related Intracoronary Thrombus in a Patient with Liver Cirrhosis
Ji Woong Roh, Eun Hyea Park, Joon Cheol Song, Young Seung Oh, Tong Yoon Kim, Hyo Suk Kim, Sungmin Lim
Korean J Crit Care Med. 2015;30(4):358-364. doi: 10.4266/kjccm.2015.30.4.358.
Reference
-
1. Hartnell GG, Parnell BM, Pridie RB. Coronary artery ectasia. Its prevalence and clinical significance in 4993 patients. Br Heart J. 1985. 54:392–395.
Article2. Swaye PS, Fisher LD, Litwin P, Vignola PA, Judkins MP, Kemp HG, et al. Aneurysmal coronary artery disease. Circulation. 1983. 67:134–138.
Article3. Dogan A, Ozaydin M, Gedikli O, Altinbas A, Ergene O. Effect of trimetazidine on exercise performance in patients with coronary artery ectasia. Jpn Heart J. 2003. 44:463–470.
Article4. Sorrell VL, Davis MJ, Bove AA. Current knowledge and significance of coronary artery ectasia: a chronologic review of the literature, recommendations for treatment, possible etiologies, and future considerations. Clin Cardiol. 1998. 21:157–160.
Article5. Fineschi M, Gori T, Sinicropi G, Bravi A. Polytetrafluoroethylene (PTFE) covered stents for the treatment of coronary artery aneurysms. Heart. 2004. 90:490.
Article6. Burzotta F, Trani C, Romagnoli E, Mazzari MA, Savino M, Schiavoni G, et al. Percutaneous treatment of a large coronary aneurysm using the self-expandable Symbiot PTFE-covered stent. Chest. 2004. 126:644–645.
Article7. Bricker DL, Rittmann DV Jr. Arteriosclerotic aneurysms of the coronary arteries: surgical treatment. Tex Heart Inst J. 1987. 14:23–30.8. Agirbasli M, Morris DC, Marshall JJ. The use of intrastent peripheral stent in large coronary arteries: report of three cases. Catheter Cardiovasc Interv. 2000. 50:498–501.
Article9. Stefanadis C, Toutouzas K, Tsiamis E, Toutouzas P. New stent design for autologous venous graft-covered stent preparation: first human application for sealing of a coronary aneurysm. Catheter Cardiovasc Interv. 2002. 55:222–227.
Article10. Rha SW, Wani SP, Oh DJ. Parallel stenting using two sirolimus-eluting stents in an ectatic coronary artery stenosis. Heart. 2007. 93:976.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Percutaneous Transluminal Coronary Angioplasty for Coronary Artery Stenosis in an Adult Kawasaki Disease with Coronary Aneurysm : A Case Report and Review
- Onlay Patch Coronary Angioplasty with Autologous Saphenous Vein
- Stenting of the Left Main Coronary Artery in a Patient With Takayasu's Arteritis
- Aspiration Thromboembolectomy in the Management of Acute Coronary Occlusion during Pertaneous Transluminal Coronary Angioplasty
- Percutaneous transluminal coronary angioplasty for ostial stenosis of the left coronary artery
